Annie E. Larson, Kurt C. Stange, John Heintzman, Yui Nishiike, Brenda M. McGrath, Melinda M. Davis, S. Marie Harvey
{"title":"从电子健康记录数据中识别虚拟护理模式","authors":"Annie E. Larson, Kurt C. Stange, John Heintzman, Yui Nishiike, Brenda M. McGrath, Melinda M. Davis, S. Marie Harvey","doi":"10.1002/lrh2.10411","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Virtual care increased dramatically during the COVID-19 pandemic. The specific modality of virtual care (video, audio, eVisits, eConsults, and remote patient monitoring) has important implications for the accessibility and quality of care, but rates of use are relatively unknown. Methods for identifying virtual care modalities, especially in electronic health records (EHR) are inconsistent. This study (a) developed a method to identify virtual care modalities using EHR data and (b) described the distribution of these modalities over a 3-year study period.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>EHR data from 316 primary care safety net clinics throughout the study period (4/1/2020-3/31/2023) were included. Visit type (in-person vs virtual) by adults >18 years old were classified. Expert consultation informed the development of two algorithms to classify virtual care visit modalities; these algorithms prioritized different EHR data elements. We conducted descriptive analyses comparing algorithms and the frequency of virtual care modalities.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Agreement between the algorithms was 96.5% for all visits and 89.3% for virtual care visits. The majority of disagreement between the algorithms was among encounters scheduled as audio-only but billed as a video visit. Restricting to visits where the algorithms agreed on visit modality, there were 2-fold more audio-only than video visits.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Visit modality classification varies depending upon which data in the EHR are prioritized. Regardless of which algorithm is utilized, safety net clinics rely on audio-only and video visits to provide care in virtual visits. Elimination of reimbursement for audio visits may exacerbate existing inequities in care for low-income patients.</p>\n </section>\n </div>","PeriodicalId":43916,"journal":{"name":"Learning Health Systems","volume":"8 S1","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10411","citationCount":"0","resultStr":"{\"title\":\"Identifying virtual care modality in electronic health record data\",\"authors\":\"Annie E. Larson, Kurt C. Stange, John Heintzman, Yui Nishiike, Brenda M. McGrath, Melinda M. Davis, S. Marie Harvey\",\"doi\":\"10.1002/lrh2.10411\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Virtual care increased dramatically during the COVID-19 pandemic. The specific modality of virtual care (video, audio, eVisits, eConsults, and remote patient monitoring) has important implications for the accessibility and quality of care, but rates of use are relatively unknown. Methods for identifying virtual care modalities, especially in electronic health records (EHR) are inconsistent. This study (a) developed a method to identify virtual care modalities using EHR data and (b) described the distribution of these modalities over a 3-year study period.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>EHR data from 316 primary care safety net clinics throughout the study period (4/1/2020-3/31/2023) were included. Visit type (in-person vs virtual) by adults >18 years old were classified. Expert consultation informed the development of two algorithms to classify virtual care visit modalities; these algorithms prioritized different EHR data elements. We conducted descriptive analyses comparing algorithms and the frequency of virtual care modalities.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Agreement between the algorithms was 96.5% for all visits and 89.3% for virtual care visits. The majority of disagreement between the algorithms was among encounters scheduled as audio-only but billed as a video visit. Restricting to visits where the algorithms agreed on visit modality, there were 2-fold more audio-only than video visits.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Visit modality classification varies depending upon which data in the EHR are prioritized. Regardless of which algorithm is utilized, safety net clinics rely on audio-only and video visits to provide care in virtual visits. Elimination of reimbursement for audio visits may exacerbate existing inequities in care for low-income patients.</p>\\n </section>\\n </div>\",\"PeriodicalId\":43916,\"journal\":{\"name\":\"Learning Health Systems\",\"volume\":\"8 S1\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-02-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10411\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Learning Health Systems\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10411\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Learning Health Systems","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10411","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
Identifying virtual care modality in electronic health record data
Background
Virtual care increased dramatically during the COVID-19 pandemic. The specific modality of virtual care (video, audio, eVisits, eConsults, and remote patient monitoring) has important implications for the accessibility and quality of care, but rates of use are relatively unknown. Methods for identifying virtual care modalities, especially in electronic health records (EHR) are inconsistent. This study (a) developed a method to identify virtual care modalities using EHR data and (b) described the distribution of these modalities over a 3-year study period.
Methods
EHR data from 316 primary care safety net clinics throughout the study period (4/1/2020-3/31/2023) were included. Visit type (in-person vs virtual) by adults >18 years old were classified. Expert consultation informed the development of two algorithms to classify virtual care visit modalities; these algorithms prioritized different EHR data elements. We conducted descriptive analyses comparing algorithms and the frequency of virtual care modalities.
Results
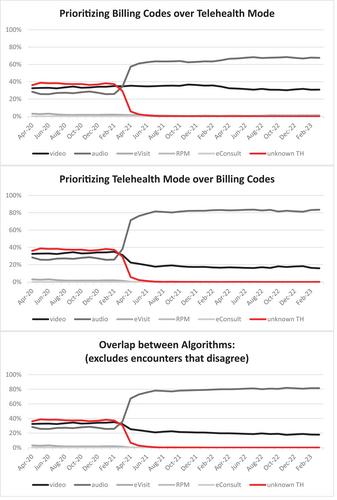
Agreement between the algorithms was 96.5% for all visits and 89.3% for virtual care visits. The majority of disagreement between the algorithms was among encounters scheduled as audio-only but billed as a video visit. Restricting to visits where the algorithms agreed on visit modality, there were 2-fold more audio-only than video visits.
Conclusion
Visit modality classification varies depending upon which data in the EHR are prioritized. Regardless of which algorithm is utilized, safety net clinics rely on audio-only and video visits to provide care in virtual visits. Elimination of reimbursement for audio visits may exacerbate existing inequities in care for low-income patients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
