{"title":"肥大细胞白血病中的 II 型肥大细胞:不常见但临床意义重大","authors":"Constance P. Chen, Dong Chen","doi":"10.1002/jha2.893","DOIUrl":null,"url":null,"abstract":"<p>A 41-year-old female patient with a past medical history of cutaneous mastocytosis presented with musculoskeletal pain. A whole-body positron emission tomography-computed tomography scan showed diffuse bone marrow (BM) fluorodeoxyglucose uptake, most prominent in the humerus and femur. Her complete blood count showed hemoglobin, 7.2 g/dL; white blood cells, 9.8 × 10<sup>9</sup>/L with eosinophilia (2.79 × 10<sup>9</sup>/L); neutrophils, 4.4 × 10<sup>9</sup>/L; lymphocytes, 2.16 × 10<sup>9</sup>/L; monocytes, 0.37 × 10<sup>9</sup>/L; basophils, 0.03 × 10<sup>9</sup>/L and platelets, 179 × 10<sup>9</sup>/L. Her Wright-Giemsa (WG)-stained peripheral blood showed normal-appearing eosinophils without circulating blasts, atypical lymphocytes, or mast cells (MCs). Her WG-stained BM aspirate smears (Figure 1A and 1B) and Hematoxylin-eosin-stained BM biopsy sections (Figure 1C) revealed 80% of cytologically atypical MCs. These MCs exhibited distinct bilobed or multi-lobed nuclei and metachromatic intracytoplasmic granules, morphologically consistent with type II (immature) MCs (denoted with asterisks at 1000X magnification in Panels A–C). They expressed CD25, CD117, and tryptase by immunohistochemical stains and were positive for <i>KIT</i> D816V (variant allele frequency [VAF], 11%) and <i>DNMT3A</i> R899C (VAF, 46%) mutations by a next-generation sequencing study. The cytogenetic study result was normal. The residual trilineage hematopoiesis was markedly decreased with normal morphology. The patient was diagnosed with MC leukemia (MCL) and was refractory to multiple lines of therapy, including Avapritinib.</p><p>As shown in this case, it is essential to recognize the type II MCs for both diagnosis and prognostification of MCL. Although this case fulfilled the diagnostic criteria of MCL by both the International Consensus Classification (ICC) and the 5th World Health Organization Classification, the ICC specifically requires more than 20% type II (immature) MCs on the BM smear or biopsy. MCL patients with increased type II MCs often have much worse clinical outcomes.</p><p>Constance Chen drafted the manuscript and made the figure. Dong Chen drafted the manuscript and provided the pathology images of this case.</p><p>The authors declare no conflict of interest.</p><p>The authors have confirmed ethical approval statement is not needed for this submission.</p><p>The authors have confirmed patient consent statement is not needed for this submission.</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>","PeriodicalId":72883,"journal":{"name":"EJHaem","volume":"5 2","pages":"412-413"},"PeriodicalIF":1.2000,"publicationDate":"2024-04-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.893","citationCount":"0","resultStr":"{\"title\":\"Type II mast cells in mast cell leukemia: Uncommon yet clinically significant\",\"authors\":\"Constance P. Chen, Dong Chen\",\"doi\":\"10.1002/jha2.893\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 41-year-old female patient with a past medical history of cutaneous mastocytosis presented with musculoskeletal pain. A whole-body positron emission tomography-computed tomography scan showed diffuse bone marrow (BM) fluorodeoxyglucose uptake, most prominent in the humerus and femur. Her complete blood count showed hemoglobin, 7.2 g/dL; white blood cells, 9.8 × 10<sup>9</sup>/L with eosinophilia (2.79 × 10<sup>9</sup>/L); neutrophils, 4.4 × 10<sup>9</sup>/L; lymphocytes, 2.16 × 10<sup>9</sup>/L; monocytes, 0.37 × 10<sup>9</sup>/L; basophils, 0.03 × 10<sup>9</sup>/L and platelets, 179 × 10<sup>9</sup>/L. Her Wright-Giemsa (WG)-stained peripheral blood showed normal-appearing eosinophils without circulating blasts, atypical lymphocytes, or mast cells (MCs). Her WG-stained BM aspirate smears (Figure 1A and 1B) and Hematoxylin-eosin-stained BM biopsy sections (Figure 1C) revealed 80% of cytologically atypical MCs. These MCs exhibited distinct bilobed or multi-lobed nuclei and metachromatic intracytoplasmic granules, morphologically consistent with type II (immature) MCs (denoted with asterisks at 1000X magnification in Panels A–C). They expressed CD25, CD117, and tryptase by immunohistochemical stains and were positive for <i>KIT</i> D816V (variant allele frequency [VAF], 11%) and <i>DNMT3A</i> R899C (VAF, 46%) mutations by a next-generation sequencing study. The cytogenetic study result was normal. The residual trilineage hematopoiesis was markedly decreased with normal morphology. The patient was diagnosed with MC leukemia (MCL) and was refractory to multiple lines of therapy, including Avapritinib.</p><p>As shown in this case, it is essential to recognize the type II MCs for both diagnosis and prognostification of MCL. Although this case fulfilled the diagnostic criteria of MCL by both the International Consensus Classification (ICC) and the 5th World Health Organization Classification, the ICC specifically requires more than 20% type II (immature) MCs on the BM smear or biopsy. MCL patients with increased type II MCs often have much worse clinical outcomes.</p><p>Constance Chen drafted the manuscript and made the figure. Dong Chen drafted the manuscript and provided the pathology images of this case.</p><p>The authors declare no conflict of interest.</p><p>The authors have confirmed ethical approval statement is not needed for this submission.</p><p>The authors have confirmed patient consent statement is not needed for this submission.</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>\",\"PeriodicalId\":72883,\"journal\":{\"name\":\"EJHaem\",\"volume\":\"5 2\",\"pages\":\"412-413\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-04-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.893\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"EJHaem\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jha2.893\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"EJHaem","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jha2.893","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Type II mast cells in mast cell leukemia: Uncommon yet clinically significant
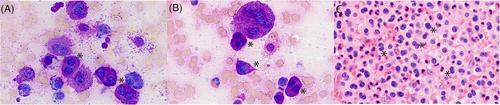
A 41-year-old female patient with a past medical history of cutaneous mastocytosis presented with musculoskeletal pain. A whole-body positron emission tomography-computed tomography scan showed diffuse bone marrow (BM) fluorodeoxyglucose uptake, most prominent in the humerus and femur. Her complete blood count showed hemoglobin, 7.2 g/dL; white blood cells, 9.8 × 109/L with eosinophilia (2.79 × 109/L); neutrophils, 4.4 × 109/L; lymphocytes, 2.16 × 109/L; monocytes, 0.37 × 109/L; basophils, 0.03 × 109/L and platelets, 179 × 109/L. Her Wright-Giemsa (WG)-stained peripheral blood showed normal-appearing eosinophils without circulating blasts, atypical lymphocytes, or mast cells (MCs). Her WG-stained BM aspirate smears (Figure 1A and 1B) and Hematoxylin-eosin-stained BM biopsy sections (Figure 1C) revealed 80% of cytologically atypical MCs. These MCs exhibited distinct bilobed or multi-lobed nuclei and metachromatic intracytoplasmic granules, morphologically consistent with type II (immature) MCs (denoted with asterisks at 1000X magnification in Panels A–C). They expressed CD25, CD117, and tryptase by immunohistochemical stains and were positive for KIT D816V (variant allele frequency [VAF], 11%) and DNMT3A R899C (VAF, 46%) mutations by a next-generation sequencing study. The cytogenetic study result was normal. The residual trilineage hematopoiesis was markedly decreased with normal morphology. The patient was diagnosed with MC leukemia (MCL) and was refractory to multiple lines of therapy, including Avapritinib.
As shown in this case, it is essential to recognize the type II MCs for both diagnosis and prognostification of MCL. Although this case fulfilled the diagnostic criteria of MCL by both the International Consensus Classification (ICC) and the 5th World Health Organization Classification, the ICC specifically requires more than 20% type II (immature) MCs on the BM smear or biopsy. MCL patients with increased type II MCs often have much worse clinical outcomes.
Constance Chen drafted the manuscript and made the figure. Dong Chen drafted the manuscript and provided the pathology images of this case.
The authors declare no conflict of interest.
The authors have confirmed ethical approval statement is not needed for this submission.
The authors have confirmed patient consent statement is not needed for this submission.
The authors have confirmed clinical trial registration is not needed for this submission.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
