Olivia Magwood, Ammar Saad, Dominique Ranger, Kate Volpini, Franklin Rukikamirera, Rinila Haridas, Shahab Sayfi, Jeremie Alexander, Yvonne Tan, Kevin Pottie
{"title":"减少青少年抑郁症状和饮酒的手机应用:系统综述和荟萃分析:系统综述","authors":"Olivia Magwood, Ammar Saad, Dominique Ranger, Kate Volpini, Franklin Rukikamirera, Rinila Haridas, Shahab Sayfi, Jeremie Alexander, Yvonne Tan, Kevin Pottie","doi":"10.1002/cl2.1398","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Among youth, symptoms of depression, anxiety, and alcohol use are associated with considerable illness and disability. Youth face many personal and health system barriers in accessing mental health care. Mobile applications (apps) offer youth potentially accessible, scalable, and anonymous therapy and other support. Recent systematic reviews on apps to reduce mental health symptoms among youth have reported uncertain effectiveness, but analyses based on the type of app-delivered therapy are limited.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>We conducted this systematic review with youth co-researchers to ensure that this review addressed the questions that were most important to them. The objective of this review is to synthesize the best available evidence on the effectiveness of mobile apps for the reduction of depressive symptoms (depression, generalized anxiety, psychological distress) and alcohol use among youth.</p>\n </section>\n \n <section>\n \n <h3> Search Methods</h3>\n \n <p>We conducted electronic searches of the following bibliographic databases for studies published between January 1, 2008, and July 1, 2022: MEDLINE (via Ovid), Embase (via Ovid), PsycINFO (via Ovid), CINAHL (via EBSCOHost), and CENTRAL (via the Cochrane Library). The search used a combination of indexed terms, free text words, and MeSH headings. We manually screened the references of relevant systematic reviews and included randomized controlled trials (RCTs) for additional eligible studies, and contacted authors for full reports of identified trial registries or protocols.</p>\n </section>\n \n <section>\n \n <h3> Selection Criteria</h3>\n \n <p>We included RCTs conducted among youth aged 15–24 years from any setting. We did not exclude populations on the basis of gender, socioeconomic status, geographic location or other personal characteristics. We included studies which assessed the effectiveness of app-delivered mental health support or therapy interventions that targeted the management of depressive disorders and/or alcohol use disorders. We excluded apps that targeted general wellness, apps which focused on prevention of psychological disorders and apps that targeted bipolar disorder, psychosis, post-traumatic stress disorder, attention-deficit hyperactivity disorder, substance use disorders (aside from alcohol), and sleep disorders. Eligible comparisons included usual care, no intervention, wait-list control, alternative or controlled mobile applications. We included studies which reported outcomes on depressive symptoms, anxiety symptoms, alcohol use and psychological distress over any follow-up period.</p>\n </section>\n \n <section>\n \n <h3> Data Collection and Analysis</h3>\n \n <p>We standardized the PICO definitions (population, intervention, comparison, and outcome) of each included study and grouped studies by the type of therapy or support offered by the app. Whenever app design and clinical homogeneity allowed, we meta-analyzed outcomes using a random-effects model. Outcome data measured using categorical scales were synthesized using odds ratios. Outcome data measured using continuous scales were synthesized as the standardized mean difference. We assessed the methodological quality of each included study using the Cochrane Risk of Bias 2.0 tool and we assessed certainty of the evidence using the GRADE approach.</p>\n </section>\n \n <section>\n \n <h3> Main Results</h3>\n \n <p>From 5280 unique citations, we included 36 RCTs published in 37 reports and conducted in 15 different countries (7984 participants). Among the 36 included trials, we assessed two with an overall low risk of bias, 8 trials with some concern regarding risk of bias, and 26 trials with a high risk of bias. Interventions varied in the type of therapy or supports offered. The most common intervention designs employed mindfulness training, cognitive behavioral therapy (CBT), or a combination of the two (mindfulness + CBT). However, other interventions also included self-monitoring, medication reminders, cognitive bias modification or positive stimulation, dialectical behavioral therapy, gamified health promotion, or social skill building. Mindfulness apps led to short term improvements in depressive symptoms when compared to a withheld control (SMD = −0.36; 95% CI [−0.63, −0.10]; <i>p</i> = 0.007, <i>n</i> = 3 RCTs, GRADE: very low certainty) and when compared to an active control (SMD = −0.27; 95% CI [−0.53, −0.01]; <i>p</i> = 0.04, <i>n</i> = 2 RCTs, GRADE: very low). Apps delivering this type of support also significantly improved symptoms of anxiety when compared to a withheld control (SMD = −0.35; 95% CI [−0.60, −0.09]; <i>p</i> = 0.008, <i>n</i> = 3 RCTs, GRADE: very low) but not when compared to an active control (SMD = −0.24; 95% CI [−0.50, 0.02]; <i>p</i> = 0.07, <i>n</i> = 2 RCTs, GRADE: very low). Mindfulness apps showed improvements in psychological stress that approached statistical significance among participants receiving the mindfulness mobile apps compared to those in the withheld control (SMD = −0.27; 95% CI [−0.56, 0.03]; <i>p</i> = .07, <i>n</i> = 4 RCTs, GRADE: very low). CBT apps also led to short-term improvements in depressive symptoms when compared to a withheld control (SMD = −0.40; 95% CI [−0.80, 0.01]; <i>p</i> = 0.05, <i>n</i> = 2 RCTs, GRADE: very low) and when compared to an active control (SMD = −0.59; 95% CI [−0.98, −0.19]; <i>p</i> = 0.003, <i>n</i> = 2 RCTs, GRADE: very low). CBT-based apps also improved symptoms of anxiety compared to a withheld control (SMD = −0.51; 95% CI [−0.94, −0.09]; <i>p</i> = 0.02, <i>n</i> = 3 RCTs, GRADE: very low) but not when compared to an active control (SMD = −0.26; 95% CI [−1.11, 0.59]; <i>p</i> = 0.55, <i>n</i> = 3 RCTs, GRADE: very low). Apps which combined mindfulness and CBT did not significantly improve symptoms of depression (SMD = −0.20; 95% CI [−0.42, 0.02]; <i>p</i> = 0.07, <i>n</i> = 2 RCTs, GRADE: very low) or anxiety (SMD = −0.21; 95% CI [−0.49, 0.07]; <i>p</i> = 0.14, <i>n</i> = 2 RCTs, GRADE: very low). However, these apps did improve psychological distress (SMD = −0.43; 95% CI [−0.74, −0.12]; <i>p</i> = 0.006, <i>n</i> = 2 RCTs, GRADE: very low). The results of trials on apps to reduce alcohol use were inconsistent. We did not identify any harms associated with the use of apps to manage mental health concerns. All effectiveness results had a very low certainty of evidence rating using the GRADE approach, meaning that apps which deliver therapy or other mental health support may reduce symptoms of depression, anxiety and psychological distress but the evidence is very uncertain.</p>\n </section>\n \n <section>\n \n <h3> Authors' Conclusions</h3>\n \n <p>We reviewed evidence from 36 trials conducted among youth. According to our meta-analyses, the evidence is very uncertain about the effect of apps on depression, anxiety, psychological distress, and alcohol use. Very few effects were interpreted to be of clinical importance. Most of the RCTs were small studies focusing on efficacy for youth at risk for depressive symptoms. Larger trials are needed to evaluate effectiveness and allow for further analysis of subgroup differences. Longer trials are also needed to better estimate the clinical importance of these apps over the long term.</p>\n </section>\n </div>","PeriodicalId":36698,"journal":{"name":"Campbell Systematic Reviews","volume":"20 2","pages":""},"PeriodicalIF":7.1000,"publicationDate":"2024-04-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cl2.1398","citationCount":"0","resultStr":"{\"title\":\"Mobile apps to reduce depressive symptoms and alcohol use in youth: A systematic review and meta-analysis: A systematic review\",\"authors\":\"Olivia Magwood, Ammar Saad, Dominique Ranger, Kate Volpini, Franklin Rukikamirera, Rinila Haridas, Shahab Sayfi, Jeremie Alexander, Yvonne Tan, Kevin Pottie\",\"doi\":\"10.1002/cl2.1398\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Among youth, symptoms of depression, anxiety, and alcohol use are associated with considerable illness and disability. Youth face many personal and health system barriers in accessing mental health care. Mobile applications (apps) offer youth potentially accessible, scalable, and anonymous therapy and other support. Recent systematic reviews on apps to reduce mental health symptoms among youth have reported uncertain effectiveness, but analyses based on the type of app-delivered therapy are limited.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>We conducted this systematic review with youth co-researchers to ensure that this review addressed the questions that were most important to them. The objective of this review is to synthesize the best available evidence on the effectiveness of mobile apps for the reduction of depressive symptoms (depression, generalized anxiety, psychological distress) and alcohol use among youth.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Search Methods</h3>\\n \\n <p>We conducted electronic searches of the following bibliographic databases for studies published between January 1, 2008, and July 1, 2022: MEDLINE (via Ovid), Embase (via Ovid), PsycINFO (via Ovid), CINAHL (via EBSCOHost), and CENTRAL (via the Cochrane Library). The search used a combination of indexed terms, free text words, and MeSH headings. We manually screened the references of relevant systematic reviews and included randomized controlled trials (RCTs) for additional eligible studies, and contacted authors for full reports of identified trial registries or protocols.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Selection Criteria</h3>\\n \\n <p>We included RCTs conducted among youth aged 15–24 years from any setting. We did not exclude populations on the basis of gender, socioeconomic status, geographic location or other personal characteristics. We included studies which assessed the effectiveness of app-delivered mental health support or therapy interventions that targeted the management of depressive disorders and/or alcohol use disorders. We excluded apps that targeted general wellness, apps which focused on prevention of psychological disorders and apps that targeted bipolar disorder, psychosis, post-traumatic stress disorder, attention-deficit hyperactivity disorder, substance use disorders (aside from alcohol), and sleep disorders. Eligible comparisons included usual care, no intervention, wait-list control, alternative or controlled mobile applications. We included studies which reported outcomes on depressive symptoms, anxiety symptoms, alcohol use and psychological distress over any follow-up period.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Data Collection and Analysis</h3>\\n \\n <p>We standardized the PICO definitions (population, intervention, comparison, and outcome) of each included study and grouped studies by the type of therapy or support offered by the app. Whenever app design and clinical homogeneity allowed, we meta-analyzed outcomes using a random-effects model. Outcome data measured using categorical scales were synthesized using odds ratios. Outcome data measured using continuous scales were synthesized as the standardized mean difference. We assessed the methodological quality of each included study using the Cochrane Risk of Bias 2.0 tool and we assessed certainty of the evidence using the GRADE approach.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Main Results</h3>\\n \\n <p>From 5280 unique citations, we included 36 RCTs published in 37 reports and conducted in 15 different countries (7984 participants). Among the 36 included trials, we assessed two with an overall low risk of bias, 8 trials with some concern regarding risk of bias, and 26 trials with a high risk of bias. Interventions varied in the type of therapy or supports offered. The most common intervention designs employed mindfulness training, cognitive behavioral therapy (CBT), or a combination of the two (mindfulness + CBT). However, other interventions also included self-monitoring, medication reminders, cognitive bias modification or positive stimulation, dialectical behavioral therapy, gamified health promotion, or social skill building. Mindfulness apps led to short term improvements in depressive symptoms when compared to a withheld control (SMD = −0.36; 95% CI [−0.63, −0.10]; <i>p</i> = 0.007, <i>n</i> = 3 RCTs, GRADE: very low certainty) and when compared to an active control (SMD = −0.27; 95% CI [−0.53, −0.01]; <i>p</i> = 0.04, <i>n</i> = 2 RCTs, GRADE: very low). Apps delivering this type of support also significantly improved symptoms of anxiety when compared to a withheld control (SMD = −0.35; 95% CI [−0.60, −0.09]; <i>p</i> = 0.008, <i>n</i> = 3 RCTs, GRADE: very low) but not when compared to an active control (SMD = −0.24; 95% CI [−0.50, 0.02]; <i>p</i> = 0.07, <i>n</i> = 2 RCTs, GRADE: very low). Mindfulness apps showed improvements in psychological stress that approached statistical significance among participants receiving the mindfulness mobile apps compared to those in the withheld control (SMD = −0.27; 95% CI [−0.56, 0.03]; <i>p</i> = .07, <i>n</i> = 4 RCTs, GRADE: very low). CBT apps also led to short-term improvements in depressive symptoms when compared to a withheld control (SMD = −0.40; 95% CI [−0.80, 0.01]; <i>p</i> = 0.05, <i>n</i> = 2 RCTs, GRADE: very low) and when compared to an active control (SMD = −0.59; 95% CI [−0.98, −0.19]; <i>p</i> = 0.003, <i>n</i> = 2 RCTs, GRADE: very low). CBT-based apps also improved symptoms of anxiety compared to a withheld control (SMD = −0.51; 95% CI [−0.94, −0.09]; <i>p</i> = 0.02, <i>n</i> = 3 RCTs, GRADE: very low) but not when compared to an active control (SMD = −0.26; 95% CI [−1.11, 0.59]; <i>p</i> = 0.55, <i>n</i> = 3 RCTs, GRADE: very low). Apps which combined mindfulness and CBT did not significantly improve symptoms of depression (SMD = −0.20; 95% CI [−0.42, 0.02]; <i>p</i> = 0.07, <i>n</i> = 2 RCTs, GRADE: very low) or anxiety (SMD = −0.21; 95% CI [−0.49, 0.07]; <i>p</i> = 0.14, <i>n</i> = 2 RCTs, GRADE: very low). However, these apps did improve psychological distress (SMD = −0.43; 95% CI [−0.74, −0.12]; <i>p</i> = 0.006, <i>n</i> = 2 RCTs, GRADE: very low). The results of trials on apps to reduce alcohol use were inconsistent. We did not identify any harms associated with the use of apps to manage mental health concerns. All effectiveness results had a very low certainty of evidence rating using the GRADE approach, meaning that apps which deliver therapy or other mental health support may reduce symptoms of depression, anxiety and psychological distress but the evidence is very uncertain.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Authors' Conclusions</h3>\\n \\n <p>We reviewed evidence from 36 trials conducted among youth. According to our meta-analyses, the evidence is very uncertain about the effect of apps on depression, anxiety, psychological distress, and alcohol use. Very few effects were interpreted to be of clinical importance. Most of the RCTs were small studies focusing on efficacy for youth at risk for depressive symptoms. Larger trials are needed to evaluate effectiveness and allow for further analysis of subgroup differences. Longer trials are also needed to better estimate the clinical importance of these apps over the long term.</p>\\n </section>\\n </div>\",\"PeriodicalId\":36698,\"journal\":{\"name\":\"Campbell Systematic Reviews\",\"volume\":\"20 2\",\"pages\":\"\"},\"PeriodicalIF\":7.1000,\"publicationDate\":\"2024-04-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cl2.1398\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Campbell Systematic Reviews\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cl2.1398\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SOCIAL SCIENCES, INTERDISCIPLINARY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Campbell Systematic Reviews","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cl2.1398","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SOCIAL SCIENCES, INTERDISCIPLINARY","Score":null,"Total":0}
Mobile apps to reduce depressive symptoms and alcohol use in youth: A systematic review and meta-analysis: A systematic review
Background
Among youth, symptoms of depression, anxiety, and alcohol use are associated with considerable illness and disability. Youth face many personal and health system barriers in accessing mental health care. Mobile applications (apps) offer youth potentially accessible, scalable, and anonymous therapy and other support. Recent systematic reviews on apps to reduce mental health symptoms among youth have reported uncertain effectiveness, but analyses based on the type of app-delivered therapy are limited.
Objectives
We conducted this systematic review with youth co-researchers to ensure that this review addressed the questions that were most important to them. The objective of this review is to synthesize the best available evidence on the effectiveness of mobile apps for the reduction of depressive symptoms (depression, generalized anxiety, psychological distress) and alcohol use among youth.
Search Methods
We conducted electronic searches of the following bibliographic databases for studies published between January 1, 2008, and July 1, 2022: MEDLINE (via Ovid), Embase (via Ovid), PsycINFO (via Ovid), CINAHL (via EBSCOHost), and CENTRAL (via the Cochrane Library). The search used a combination of indexed terms, free text words, and MeSH headings. We manually screened the references of relevant systematic reviews and included randomized controlled trials (RCTs) for additional eligible studies, and contacted authors for full reports of identified trial registries or protocols.
Selection Criteria
We included RCTs conducted among youth aged 15–24 years from any setting. We did not exclude populations on the basis of gender, socioeconomic status, geographic location or other personal characteristics. We included studies which assessed the effectiveness of app-delivered mental health support or therapy interventions that targeted the management of depressive disorders and/or alcohol use disorders. We excluded apps that targeted general wellness, apps which focused on prevention of psychological disorders and apps that targeted bipolar disorder, psychosis, post-traumatic stress disorder, attention-deficit hyperactivity disorder, substance use disorders (aside from alcohol), and sleep disorders. Eligible comparisons included usual care, no intervention, wait-list control, alternative or controlled mobile applications. We included studies which reported outcomes on depressive symptoms, anxiety symptoms, alcohol use and psychological distress over any follow-up period.
Data Collection and Analysis
We standardized the PICO definitions (population, intervention, comparison, and outcome) of each included study and grouped studies by the type of therapy or support offered by the app. Whenever app design and clinical homogeneity allowed, we meta-analyzed outcomes using a random-effects model. Outcome data measured using categorical scales were synthesized using odds ratios. Outcome data measured using continuous scales were synthesized as the standardized mean difference. We assessed the methodological quality of each included study using the Cochrane Risk of Bias 2.0 tool and we assessed certainty of the evidence using the GRADE approach.
Main Results
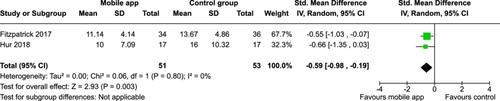
From 5280 unique citations, we included 36 RCTs published in 37 reports and conducted in 15 different countries (7984 participants). Among the 36 included trials, we assessed two with an overall low risk of bias, 8 trials with some concern regarding risk of bias, and 26 trials with a high risk of bias. Interventions varied in the type of therapy or supports offered. The most common intervention designs employed mindfulness training, cognitive behavioral therapy (CBT), or a combination of the two (mindfulness + CBT). However, other interventions also included self-monitoring, medication reminders, cognitive bias modification or positive stimulation, dialectical behavioral therapy, gamified health promotion, or social skill building. Mindfulness apps led to short term improvements in depressive symptoms when compared to a withheld control (SMD = −0.36; 95% CI [−0.63, −0.10]; p = 0.007, n = 3 RCTs, GRADE: very low certainty) and when compared to an active control (SMD = −0.27; 95% CI [−0.53, −0.01]; p = 0.04, n = 2 RCTs, GRADE: very low). Apps delivering this type of support also significantly improved symptoms of anxiety when compared to a withheld control (SMD = −0.35; 95% CI [−0.60, −0.09]; p = 0.008, n = 3 RCTs, GRADE: very low) but not when compared to an active control (SMD = −0.24; 95% CI [−0.50, 0.02]; p = 0.07, n = 2 RCTs, GRADE: very low). Mindfulness apps showed improvements in psychological stress that approached statistical significance among participants receiving the mindfulness mobile apps compared to those in the withheld control (SMD = −0.27; 95% CI [−0.56, 0.03]; p = .07, n = 4 RCTs, GRADE: very low). CBT apps also led to short-term improvements in depressive symptoms when compared to a withheld control (SMD = −0.40; 95% CI [−0.80, 0.01]; p = 0.05, n = 2 RCTs, GRADE: very low) and when compared to an active control (SMD = −0.59; 95% CI [−0.98, −0.19]; p = 0.003, n = 2 RCTs, GRADE: very low). CBT-based apps also improved symptoms of anxiety compared to a withheld control (SMD = −0.51; 95% CI [−0.94, −0.09]; p = 0.02, n = 3 RCTs, GRADE: very low) but not when compared to an active control (SMD = −0.26; 95% CI [−1.11, 0.59]; p = 0.55, n = 3 RCTs, GRADE: very low). Apps which combined mindfulness and CBT did not significantly improve symptoms of depression (SMD = −0.20; 95% CI [−0.42, 0.02]; p = 0.07, n = 2 RCTs, GRADE: very low) or anxiety (SMD = −0.21; 95% CI [−0.49, 0.07]; p = 0.14, n = 2 RCTs, GRADE: very low). However, these apps did improve psychological distress (SMD = −0.43; 95% CI [−0.74, −0.12]; p = 0.006, n = 2 RCTs, GRADE: very low). The results of trials on apps to reduce alcohol use were inconsistent. We did not identify any harms associated with the use of apps to manage mental health concerns. All effectiveness results had a very low certainty of evidence rating using the GRADE approach, meaning that apps which deliver therapy or other mental health support may reduce symptoms of depression, anxiety and psychological distress but the evidence is very uncertain.
Authors' Conclusions
We reviewed evidence from 36 trials conducted among youth. According to our meta-analyses, the evidence is very uncertain about the effect of apps on depression, anxiety, psychological distress, and alcohol use. Very few effects were interpreted to be of clinical importance. Most of the RCTs were small studies focusing on efficacy for youth at risk for depressive symptoms. Larger trials are needed to evaluate effectiveness and allow for further analysis of subgroup differences. Longer trials are also needed to better estimate the clinical importance of these apps over the long term.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
