{"title":"基于日本全国数据库的肝脏手术后发病率和死亡率风险模型","authors":"Tatsuya Orimo, Shinya Hirakawa, Akinobu Taketomi, Hisateru Tachimori, Taro Oshikiri, Hiroaki Miyata, Yoshihiro Kakeji, Ken Shirabe","doi":"10.1002/ags3.12803","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>We evaluated the morbidity and mortality associated with liver surgery in Japan and developed a risk model for liver resection using information from a national database.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We retrospectively reviewed 73 861 Japanese patients who underwent hepatectomy between 2014 and 2019, using information from the National Clinical Database (NCD) registrations. The primary endpoints were 30 days and in-hospital mortality, and the secondary endpoints were postoperative complications. Logistic regression risk models for postoperative morbidity and mortality after hepatectomy were constructed based on preoperative clinical parameters and types of liver resection, and validated using a bootstrapping method.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The 30-day and in-hospital mortality rates were 0.9% and 1.7%, respectively. Trisectionectomy, hepatectomy for gallbladder cancer, hepatectomy for perihilar cholangiocarcinoma, and poor activities of daily living were statistically significant risk factors with high odds ratios for both postoperative morbidity and mortality. Internal validations indicated that the c-indices for 30-day and in-hospital mortality were 0.824 and 0.839, respectively.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>We developed a risk model for liver resection by using a national surgical database that can predict morbidity and mortality based on preoperative factors.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 5","pages":"896-916"},"PeriodicalIF":3.3000,"publicationDate":"2024-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12803","citationCount":"0","resultStr":"{\"title\":\"Risk model for morbidity and mortality following liver surgery based on a national Japanese database\",\"authors\":\"Tatsuya Orimo, Shinya Hirakawa, Akinobu Taketomi, Hisateru Tachimori, Taro Oshikiri, Hiroaki Miyata, Yoshihiro Kakeji, Ken Shirabe\",\"doi\":\"10.1002/ags3.12803\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>We evaluated the morbidity and mortality associated with liver surgery in Japan and developed a risk model for liver resection using information from a national database.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We retrospectively reviewed 73 861 Japanese patients who underwent hepatectomy between 2014 and 2019, using information from the National Clinical Database (NCD) registrations. The primary endpoints were 30 days and in-hospital mortality, and the secondary endpoints were postoperative complications. Logistic regression risk models for postoperative morbidity and mortality after hepatectomy were constructed based on preoperative clinical parameters and types of liver resection, and validated using a bootstrapping method.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The 30-day and in-hospital mortality rates were 0.9% and 1.7%, respectively. Trisectionectomy, hepatectomy for gallbladder cancer, hepatectomy for perihilar cholangiocarcinoma, and poor activities of daily living were statistically significant risk factors with high odds ratios for both postoperative morbidity and mortality. Internal validations indicated that the c-indices for 30-day and in-hospital mortality were 0.824 and 0.839, respectively.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>We developed a risk model for liver resection by using a national surgical database that can predict morbidity and mortality based on preoperative factors.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8030,\"journal\":{\"name\":\"Annals of Gastroenterological Surgery\",\"volume\":\"8 5\",\"pages\":\"896-916\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-04-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12803\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterological Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12803\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12803","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
我们利用国家临床数据库(NCD)登记的信息,对2014年至2019年期间接受肝切除术的73 861名日本患者进行了回顾性研究。主要终点是30天死亡率和院内死亡率,次要终点是术后并发症。根据术前临床参数和肝切除类型构建了肝切除术后发病率和死亡率的逻辑回归风险模型,并采用引导法进行了验证。三段切除术、胆囊癌肝切除术、肝周胆管癌肝切除术和日常生活能力差是具有统计学意义的危险因素,术后发病率和死亡率的几率都很高。内部验证结果表明,30 天死亡率和住院死亡率的 c 指数分别为 0.824 和 0.839。我们利用全国性外科数据库开发了肝切除术风险模型,该模型可根据术前因素预测发病率和死亡率。
Risk model for morbidity and mortality following liver surgery based on a national Japanese database
Aim
We evaluated the morbidity and mortality associated with liver surgery in Japan and developed a risk model for liver resection using information from a national database.
Methods
We retrospectively reviewed 73 861 Japanese patients who underwent hepatectomy between 2014 and 2019, using information from the National Clinical Database (NCD) registrations. The primary endpoints were 30 days and in-hospital mortality, and the secondary endpoints were postoperative complications. Logistic regression risk models for postoperative morbidity and mortality after hepatectomy were constructed based on preoperative clinical parameters and types of liver resection, and validated using a bootstrapping method.
Results
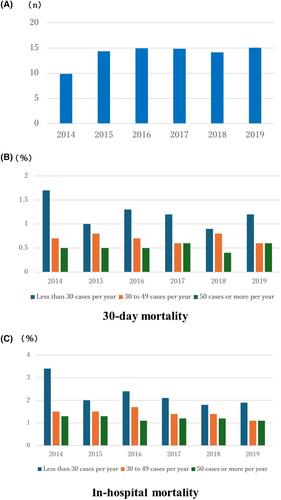
The 30-day and in-hospital mortality rates were 0.9% and 1.7%, respectively. Trisectionectomy, hepatectomy for gallbladder cancer, hepatectomy for perihilar cholangiocarcinoma, and poor activities of daily living were statistically significant risk factors with high odds ratios for both postoperative morbidity and mortality. Internal validations indicated that the c-indices for 30-day and in-hospital mortality were 0.824 and 0.839, respectively.
Conclusions
We developed a risk model for liver resection by using a national surgical database that can predict morbidity and mortality based on preoperative factors.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
