Sofie Engelen, Anne-Catherine Dens, Frederik Staels, Rik Schrijvers, Daniel Blockmans, Steven Vanderschueren, Albrecht Betrains, F. J. Sherida H. Woei-A-Jin, Arno Vanstapel, Franscesca Bosisio, Petra De Haes
{"title":"VEXAS 综合征:关注皮肤病表现及其组织病理学相关性","authors":"Sofie Engelen, Anne-Catherine Dens, Frederik Staels, Rik Schrijvers, Daniel Blockmans, Steven Vanderschueren, Albrecht Betrains, F. J. Sherida H. Woei-A-Jin, Arno Vanstapel, Franscesca Bosisio, Petra De Haes","doi":"10.1002/jvc2.395","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>VEXAS ‘Vacuoles, E1 Enzyme, X-linked, Autoinflammatory, Somatic syndrome’ is a rare autoinflammatory syndrome, first described in October 2020 by Beck et al. It is caused by somatic mutations in the <i>UBA1</i> gene, coding for the E1 enzyme, responsible for ubiquitination. It manifests in adulthood, mainly in men, with constitutional symptoms, haematological abnormalities and often skin lesions with neutrophilic dermatoses most frequently reported. Since skin lesions are a frequent and early manifestation, recognising these may prove very useful for diagnosis.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>To focus on the dermatological manifestations of VEXAS and their histopathological correlate.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We retrospectively collected data and revised skin biopsies of VEXAS patients diagnosed in our tertiary care centre, and compared those with the literature.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We identified nine men between 62 and 84 years old. The most frequently encountered <i>UBA1</i> mutation was p.Met41Thr. Skin manifestations occurred in all patients; mostly as erythematous to purpuric papules/plaques, often with annular pattern. Histopathological, early VEXAS lesions showed a gradient in infiltrate with neutrophils being concentrated in the superficial interstitium and lymphocytes situated deeper around the blood vessels. Later in the disease course, the pattern became more variable and less specific with more nuclear debris, histiocytes, neutrophils and ulceration. Haematological and constitutional manifestations were present in all patients, followed by musculoskeletal (88.8%), eye (77.7%) and cardiovascular manifestations (66.6%). Polychondritis was present in 6/9 (66.6%) patients, as were respiratory symptoms, though only 33.3% had proven lung disease. The mortality rate was 22% 10 months after diagnosis.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>This is the first cohort which describes in detail VEXAS skin manifestations with revision of all available skin biopsies, which led to the conclusion that early histopathological abnormalities in VEXAS syndrome may be easy to recognise, while the histopathological image becomes less specific over time and mimics other diseases as VEXAS progresses.</p>\n </section>\n </div>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 4","pages":"1035-1048"},"PeriodicalIF":0.5000,"publicationDate":"2024-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.395","citationCount":"0","resultStr":"{\"title\":\"VEXAS syndrome: Focus on dermatological manifestations and their histopathological correlate\",\"authors\":\"Sofie Engelen, Anne-Catherine Dens, Frederik Staels, Rik Schrijvers, Daniel Blockmans, Steven Vanderschueren, Albrecht Betrains, F. J. Sherida H. Woei-A-Jin, Arno Vanstapel, Franscesca Bosisio, Petra De Haes\",\"doi\":\"10.1002/jvc2.395\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>VEXAS ‘Vacuoles, E1 Enzyme, X-linked, Autoinflammatory, Somatic syndrome’ is a rare autoinflammatory syndrome, first described in October 2020 by Beck et al. It is caused by somatic mutations in the <i>UBA1</i> gene, coding for the E1 enzyme, responsible for ubiquitination. It manifests in adulthood, mainly in men, with constitutional symptoms, haematological abnormalities and often skin lesions with neutrophilic dermatoses most frequently reported. Since skin lesions are a frequent and early manifestation, recognising these may prove very useful for diagnosis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>To focus on the dermatological manifestations of VEXAS and their histopathological correlate.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We retrospectively collected data and revised skin biopsies of VEXAS patients diagnosed in our tertiary care centre, and compared those with the literature.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We identified nine men between 62 and 84 years old. The most frequently encountered <i>UBA1</i> mutation was p.Met41Thr. Skin manifestations occurred in all patients; mostly as erythematous to purpuric papules/plaques, often with annular pattern. Histopathological, early VEXAS lesions showed a gradient in infiltrate with neutrophils being concentrated in the superficial interstitium and lymphocytes situated deeper around the blood vessels. Later in the disease course, the pattern became more variable and less specific with more nuclear debris, histiocytes, neutrophils and ulceration. Haematological and constitutional manifestations were present in all patients, followed by musculoskeletal (88.8%), eye (77.7%) and cardiovascular manifestations (66.6%). Polychondritis was present in 6/9 (66.6%) patients, as were respiratory symptoms, though only 33.3% had proven lung disease. The mortality rate was 22% 10 months after diagnosis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>This is the first cohort which describes in detail VEXAS skin manifestations with revision of all available skin biopsies, which led to the conclusion that early histopathological abnormalities in VEXAS syndrome may be easy to recognise, while the histopathological image becomes less specific over time and mimics other diseases as VEXAS progresses.</p>\\n </section>\\n </div>\",\"PeriodicalId\":94325,\"journal\":{\"name\":\"JEADV clinical practice\",\"volume\":\"3 4\",\"pages\":\"1035-1048\"},\"PeriodicalIF\":0.5000,\"publicationDate\":\"2024-04-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.395\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JEADV clinical practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.395\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.395","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
VEXAS syndrome: Focus on dermatological manifestations and their histopathological correlate
Background
VEXAS ‘Vacuoles, E1 Enzyme, X-linked, Autoinflammatory, Somatic syndrome’ is a rare autoinflammatory syndrome, first described in October 2020 by Beck et al. It is caused by somatic mutations in the UBA1 gene, coding for the E1 enzyme, responsible for ubiquitination. It manifests in adulthood, mainly in men, with constitutional symptoms, haematological abnormalities and often skin lesions with neutrophilic dermatoses most frequently reported. Since skin lesions are a frequent and early manifestation, recognising these may prove very useful for diagnosis.
Objectives
To focus on the dermatological manifestations of VEXAS and their histopathological correlate.
Methods
We retrospectively collected data and revised skin biopsies of VEXAS patients diagnosed in our tertiary care centre, and compared those with the literature.
Results
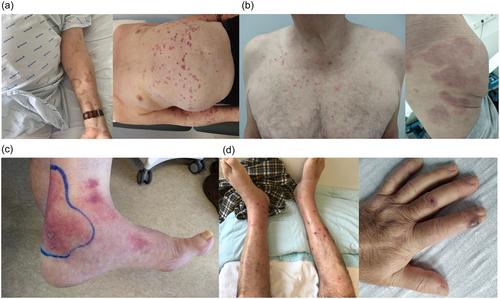
We identified nine men between 62 and 84 years old. The most frequently encountered UBA1 mutation was p.Met41Thr. Skin manifestations occurred in all patients; mostly as erythematous to purpuric papules/plaques, often with annular pattern. Histopathological, early VEXAS lesions showed a gradient in infiltrate with neutrophils being concentrated in the superficial interstitium and lymphocytes situated deeper around the blood vessels. Later in the disease course, the pattern became more variable and less specific with more nuclear debris, histiocytes, neutrophils and ulceration. Haematological and constitutional manifestations were present in all patients, followed by musculoskeletal (88.8%), eye (77.7%) and cardiovascular manifestations (66.6%). Polychondritis was present in 6/9 (66.6%) patients, as were respiratory symptoms, though only 33.3% had proven lung disease. The mortality rate was 22% 10 months after diagnosis.
Conclusions
This is the first cohort which describes in detail VEXAS skin manifestations with revision of all available skin biopsies, which led to the conclusion that early histopathological abnormalities in VEXAS syndrome may be easy to recognise, while the histopathological image becomes less specific over time and mimics other diseases as VEXAS progresses.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
