{"title":"局部晚期肺癌微创同期胸壁切除术的全国趋势、安全性和有效性","authors":"Shawn Purnell MD , Ayham Odeh MD , Richard Freeman MD, MBA , Wissam Raad MD, FACS , Elliot Servais MD, FACS , Zaid Abdelsattar MD, MS, FACS","doi":"10.1016/j.xjon.2024.03.016","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>Concomitant chest wall resection for locally advanced lung cancer is traditionally performed via an open approach. The safety and effectiveness of minimally invasive approaches for chest wall resections are unknown.</p></div><div><h3>Methods</h3><p>We used the National Cancer Database to identify patients undergoing lobectomy/bi-lobectomy with concomitant chest wall resection from 2010 to 2020. We stratified patients into those undergoing a minimally invasive resection (video-assisted thoracoscopic surgery [VATS]/robotic) or open, while accounting for conversions. We also compared VATS with robotic approaches. The main outcomes were length of stay, mortality, readmissions, and overall survival. We used multivariable, Kaplan-Meier and Cox proportional models to identify associations.</p></div><div><h3>Results</h3><p>Of 2837 patients, 756 procedures (26.6%) were started minimally invasive, of which 23.1% were robotic. There were 237 (31.3%) conversions. Patients undergoing a minimally invasive operation were similar in terms of age (65.2 ± 9.8 years vs 66.0 ± 9.9 years), sex, race, tumor histology, and location (all <em>P</em> > .05) but had smaller cancers (5.4 ± 2.6 cm vs 6.2 ± 4.3 cm; <em>P</em> < .001) compared with those undergoing open. They also had shorter length of stay (8.6 ± 7.6 days vs 9.7 ± 9.3 days; <em>P</em> < .001) but similar unadjusted 90-day mortality (8.2% vs 8.0%; <em>P</em> = .999). Neoadjuvant therapy was associated with less minimally invasive approaches (adjusted odds ratio, 0.69; <em>P</em> ≤ .001). Larger cancers were associated with less minimally invasive operations and greater rates of conversions. However, the robotic approach was associated with lower conversion rates than VATS across all tumor sizes. Overall survival was equivalent.</p></div><div><h3>Conclusions</h3><p>The use of minimally invasive approaches to concomitant chest wall resection is increasing. Although conversions to open are common, this approach is safe and is associated with shorter hospital stays. Overall survival is equivalent to the open approach.</p></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":"19 ","pages":"Pages 311-324"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2666273624000974/pdfft?md5=23e283284243639c052996ec280658de&pid=1-s2.0-S2666273624000974-main.pdf","citationCount":"0","resultStr":"{\"title\":\"National trends, safety, and effectiveness of minimally invasive concomitant chest wall resection for locally advanced lung cancer\",\"authors\":\"Shawn Purnell MD , Ayham Odeh MD , Richard Freeman MD, MBA , Wissam Raad MD, FACS , Elliot Servais MD, FACS , Zaid Abdelsattar MD, MS, FACS\",\"doi\":\"10.1016/j.xjon.2024.03.016\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>Concomitant chest wall resection for locally advanced lung cancer is traditionally performed via an open approach. The safety and effectiveness of minimally invasive approaches for chest wall resections are unknown.</p></div><div><h3>Methods</h3><p>We used the National Cancer Database to identify patients undergoing lobectomy/bi-lobectomy with concomitant chest wall resection from 2010 to 2020. We stratified patients into those undergoing a minimally invasive resection (video-assisted thoracoscopic surgery [VATS]/robotic) or open, while accounting for conversions. We also compared VATS with robotic approaches. The main outcomes were length of stay, mortality, readmissions, and overall survival. We used multivariable, Kaplan-Meier and Cox proportional models to identify associations.</p></div><div><h3>Results</h3><p>Of 2837 patients, 756 procedures (26.6%) were started minimally invasive, of which 23.1% were robotic. There were 237 (31.3%) conversions. Patients undergoing a minimally invasive operation were similar in terms of age (65.2 ± 9.8 years vs 66.0 ± 9.9 years), sex, race, tumor histology, and location (all <em>P</em> > .05) but had smaller cancers (5.4 ± 2.6 cm vs 6.2 ± 4.3 cm; <em>P</em> < .001) compared with those undergoing open. They also had shorter length of stay (8.6 ± 7.6 days vs 9.7 ± 9.3 days; <em>P</em> < .001) but similar unadjusted 90-day mortality (8.2% vs 8.0%; <em>P</em> = .999). Neoadjuvant therapy was associated with less minimally invasive approaches (adjusted odds ratio, 0.69; <em>P</em> ≤ .001). Larger cancers were associated with less minimally invasive operations and greater rates of conversions. However, the robotic approach was associated with lower conversion rates than VATS across all tumor sizes. Overall survival was equivalent.</p></div><div><h3>Conclusions</h3><p>The use of minimally invasive approaches to concomitant chest wall resection is increasing. Although conversions to open are common, this approach is safe and is associated with shorter hospital stays. Overall survival is equivalent to the open approach.</p></div>\",\"PeriodicalId\":74032,\"journal\":{\"name\":\"JTCVS open\",\"volume\":\"19 \",\"pages\":\"Pages 311-324\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2666273624000974/pdfft?md5=23e283284243639c052996ec280658de&pid=1-s2.0-S2666273624000974-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JTCVS open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666273624000974\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273624000974","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的局部晚期肺癌的胸壁同期切除术传统上是通过开放式方法进行的。方法我们利用国家癌症数据库识别了 2010 年至 2020 年期间接受肺叶切除术/双叶切除术并同时接受胸壁切除术的患者。我们将患者分为接受微创切除术(视频辅助胸腔镜手术 [VATS]/机器人手术)或开放手术的患者,同时考虑了转换手术。我们还比较了视频辅助胸腔镜手术和机器人手术。主要结果包括住院时间、死亡率、再入院率和总生存率。我们使用了多变量、Kaplan-Meier 和 Cox 比例模型来确定两者之间的关联。有 237 例(31.3%)患者转为微创手术。接受微创手术的患者在年龄(65.2 ± 9.8 岁 vs 66.0 ± 9.9 岁)、性别、种族、肿瘤组织学和位置(均为 P >.05)方面相似,但与接受开放手术的患者相比,他们的癌细胞更小(5.4 ± 2.6 cm vs 6.2 ± 4.3 cm; P <.001)。他们的住院时间也较短(8.6 ± 7.6 天 vs 9.7 ± 9.3 天;P < .001),但未经调整的 90 天死亡率相似(8.2% vs 8.0%;P = .999)。新辅助治疗与较少的微创方法有关(调整后的几率比为0.69;P≤.001)。较大的癌症与较少的微创手术和较高的转换率有关。然而,在所有大小的肿瘤中,机器人方法的转换率均低于VATS方法。结论同时进行胸壁切除术的微创方法越来越多。虽然转为开胸手术的情况很常见,但这种方法很安全,而且住院时间较短。总生存率与开放式方法相当。
National trends, safety, and effectiveness of minimally invasive concomitant chest wall resection for locally advanced lung cancer
Objective
Concomitant chest wall resection for locally advanced lung cancer is traditionally performed via an open approach. The safety and effectiveness of minimally invasive approaches for chest wall resections are unknown.
Methods
We used the National Cancer Database to identify patients undergoing lobectomy/bi-lobectomy with concomitant chest wall resection from 2010 to 2020. We stratified patients into those undergoing a minimally invasive resection (video-assisted thoracoscopic surgery [VATS]/robotic) or open, while accounting for conversions. We also compared VATS with robotic approaches. The main outcomes were length of stay, mortality, readmissions, and overall survival. We used multivariable, Kaplan-Meier and Cox proportional models to identify associations.
Results
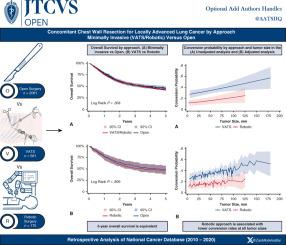
Of 2837 patients, 756 procedures (26.6%) were started minimally invasive, of which 23.1% were robotic. There were 237 (31.3%) conversions. Patients undergoing a minimally invasive operation were similar in terms of age (65.2 ± 9.8 years vs 66.0 ± 9.9 years), sex, race, tumor histology, and location (all P > .05) but had smaller cancers (5.4 ± 2.6 cm vs 6.2 ± 4.3 cm; P < .001) compared with those undergoing open. They also had shorter length of stay (8.6 ± 7.6 days vs 9.7 ± 9.3 days; P < .001) but similar unadjusted 90-day mortality (8.2% vs 8.0%; P = .999). Neoadjuvant therapy was associated with less minimally invasive approaches (adjusted odds ratio, 0.69; P ≤ .001). Larger cancers were associated with less minimally invasive operations and greater rates of conversions. However, the robotic approach was associated with lower conversion rates than VATS across all tumor sizes. Overall survival was equivalent.
Conclusions
The use of minimally invasive approaches to concomitant chest wall resection is increasing. Although conversions to open are common, this approach is safe and is associated with shorter hospital stays. Overall survival is equivalent to the open approach.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
