Mark Ayoub, Carol Faris, Julton Tomanguillo Chumbe, Ebubekir Daglilar, Nadeem Anwar, Vishnu Naravadi
{"title":"DOACs 在 Child-Pugh C 级肝硬化和试验性心颤患者中的安全性","authors":"Mark Ayoub, Carol Faris, Julton Tomanguillo Chumbe, Ebubekir Daglilar, Nadeem Anwar, Vishnu Naravadi","doi":"10.1002/jgh3.13074","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Anticoagulation (AC) is used for stroke prevention in atrial fibrillation (AF). Direct Oral Anticoagulants (DOACs) are safe in patients with AF without cirrhosis, they are hardly studied in patients with advanced cirrhosis. Our study evaluates the safety and outcomes of DOACs in patients with Child-Pugh class C cirrhosis (CPC).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We queried TriNetX Database. Patients with CPC and AF were divided into three cohorts: patients on DOACs, no AC, and warfarin. Three study arms were created using a 1:1 propensity score matching system (PSM).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Totally 16 029 patients met the inclusion criteria. Of those, 20.2% (<i>n</i> = 3235) were on DOACs, 47.1% (<i>n</i> = 7552) were not on AC, and 32.7% (<i>n</i> = 5242) were on warfarin. First arm comparing AC <i>versus</i> no AC, a statistically significant benefit was identified in 3-year mortality risk (47% <i>vs</i> 71%, <i>P</i> < 0.0001) and transplant status (17% <i>vs</i> 5%, p < 0.0001) with AC. However, no significant difference was identified regarding intracranial hemorrhage and GI bleeding risk. Second arm comparing patients on DOACs <i>versus</i> no AC, we identified mortality benefit (40% <i>vs</i> 72%, <i>P</i> < 0.0001) and a higher transplant rate (9% <i>vs</i> 3.2%, <i>P</i> < 0.0001) with DOACs. Intracranial hemorrhage rates (6% <i>vs</i> 4%, <i>P</i> = 0.03) were higher in patients on DOACs. Third arm comparing patients on DOACs <i>versus</i> Warfarin, a statistically significant lower risk of intracranial hemorrhage (6.6% <i>vs</i> 8.7%, <i>P</i> = 0.004) and GI bleed (2% <i>vs</i> 2.4%, <i>P</i> < 0.0001) were identified in patients on DOACs.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Anticoagulation is safe in patients with CPC with AF and may provide a mortality benefit. DOACs are a safer alternative to warfarin.</p>\n </section>\n </div>","PeriodicalId":45861,"journal":{"name":"JGH Open","volume":"8 5","pages":""},"PeriodicalIF":1.7000,"publicationDate":"2024-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgh3.13074","citationCount":"0","resultStr":"{\"title\":\"Safety of DOACs in patients with Child-Pugh Class C cirrhosis and trial fibrillation\",\"authors\":\"Mark Ayoub, Carol Faris, Julton Tomanguillo Chumbe, Ebubekir Daglilar, Nadeem Anwar, Vishnu Naravadi\",\"doi\":\"10.1002/jgh3.13074\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Anticoagulation (AC) is used for stroke prevention in atrial fibrillation (AF). Direct Oral Anticoagulants (DOACs) are safe in patients with AF without cirrhosis, they are hardly studied in patients with advanced cirrhosis. Our study evaluates the safety and outcomes of DOACs in patients with Child-Pugh class C cirrhosis (CPC).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We queried TriNetX Database. Patients with CPC and AF were divided into three cohorts: patients on DOACs, no AC, and warfarin. Three study arms were created using a 1:1 propensity score matching system (PSM).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Totally 16 029 patients met the inclusion criteria. Of those, 20.2% (<i>n</i> = 3235) were on DOACs, 47.1% (<i>n</i> = 7552) were not on AC, and 32.7% (<i>n</i> = 5242) were on warfarin. First arm comparing AC <i>versus</i> no AC, a statistically significant benefit was identified in 3-year mortality risk (47% <i>vs</i> 71%, <i>P</i> < 0.0001) and transplant status (17% <i>vs</i> 5%, p < 0.0001) with AC. However, no significant difference was identified regarding intracranial hemorrhage and GI bleeding risk. Second arm comparing patients on DOACs <i>versus</i> no AC, we identified mortality benefit (40% <i>vs</i> 72%, <i>P</i> < 0.0001) and a higher transplant rate (9% <i>vs</i> 3.2%, <i>P</i> < 0.0001) with DOACs. Intracranial hemorrhage rates (6% <i>vs</i> 4%, <i>P</i> = 0.03) were higher in patients on DOACs. Third arm comparing patients on DOACs <i>versus</i> Warfarin, a statistically significant lower risk of intracranial hemorrhage (6.6% <i>vs</i> 8.7%, <i>P</i> = 0.004) and GI bleed (2% <i>vs</i> 2.4%, <i>P</i> < 0.0001) were identified in patients on DOACs.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Anticoagulation is safe in patients with CPC with AF and may provide a mortality benefit. DOACs are a safer alternative to warfarin.</p>\\n </section>\\n </div>\",\"PeriodicalId\":45861,\"journal\":{\"name\":\"JGH Open\",\"volume\":\"8 5\",\"pages\":\"\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgh3.13074\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JGH Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.13074\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JGH Open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.13074","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景 抗凝(AC)用于预防房颤(AF)患者中风。直接口服抗凝药(DOACs)对未患肝硬化的房颤患者是安全的,但对晚期肝硬化患者几乎没有研究。我们的研究评估了 DOACs 在 Child-Pugh C 级肝硬化 (CPC) 患者中的安全性和疗效。 方法 我们查询了 TriNetX 数据库。CPC 和房颤患者被分为三个队列:使用 DOACs 的患者、不使用 AC 的患者和使用华法林的患者。使用 1:1 倾向评分匹配系统 (PSM) 创建了三个研究臂。 结果 共有 16 029 名患者符合纳入标准。其中,20.2%(n = 3235)使用 DOACs,47.1%(n = 7552)未使用 AC,32.7%(n = 5242)使用华法林。第一臂比较了使用 AC 与不使用 AC,发现使用 AC 在 3 年死亡风险(47% vs 71%,P < 0.0001)和移植状态(17% vs 5%,P < 0.0001)方面有显著统计学获益。但是,在颅内出血和消化道出血风险方面没有发现明显差异。第二组比较了使用 DOACs 和不使用 AC 的患者,我们发现使用 DOACs 有死亡率优势(40% vs 72%,P < 0.0001)和更高的移植率(9% vs 3.2%,P < 0.0001)。使用 DOACs 的患者颅内出血率更高(6% vs 4%,P = 0.03)。第三组将使用 DOACs 的患者与使用华法林的患者进行比较,发现使用 DOACs 的患者发生颅内出血(6.6% vs 8.7%,P = 0.004)和消化道出血(2% vs 2.4%,P < 0.0001)的风险显著低于使用华法林的患者。 结论 抗凝治疗对合并房颤的 CPC 患者是安全的,并可降低死亡率。DOACs 是一种比华法林更安全的替代药物。
Safety of DOACs in patients with Child-Pugh Class C cirrhosis and trial fibrillation
Background
Anticoagulation (AC) is used for stroke prevention in atrial fibrillation (AF). Direct Oral Anticoagulants (DOACs) are safe in patients with AF without cirrhosis, they are hardly studied in patients with advanced cirrhosis. Our study evaluates the safety and outcomes of DOACs in patients with Child-Pugh class C cirrhosis (CPC).
Methods
We queried TriNetX Database. Patients with CPC and AF were divided into three cohorts: patients on DOACs, no AC, and warfarin. Three study arms were created using a 1:1 propensity score matching system (PSM).
Results
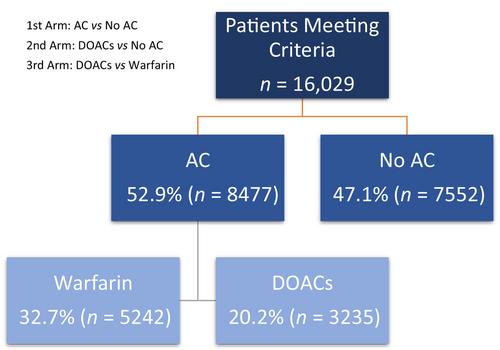
Totally 16 029 patients met the inclusion criteria. Of those, 20.2% (n = 3235) were on DOACs, 47.1% (n = 7552) were not on AC, and 32.7% (n = 5242) were on warfarin. First arm comparing AC versus no AC, a statistically significant benefit was identified in 3-year mortality risk (47% vs 71%, P < 0.0001) and transplant status (17% vs 5%, p < 0.0001) with AC. However, no significant difference was identified regarding intracranial hemorrhage and GI bleeding risk. Second arm comparing patients on DOACs versus no AC, we identified mortality benefit (40% vs 72%, P < 0.0001) and a higher transplant rate (9% vs 3.2%, P < 0.0001) with DOACs. Intracranial hemorrhage rates (6% vs 4%, P = 0.03) were higher in patients on DOACs. Third arm comparing patients on DOACs versus Warfarin, a statistically significant lower risk of intracranial hemorrhage (6.6% vs 8.7%, P = 0.004) and GI bleed (2% vs 2.4%, P < 0.0001) were identified in patients on DOACs.
Conclusion
Anticoagulation is safe in patients with CPC with AF and may provide a mortality benefit. DOACs are a safer alternative to warfarin.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
