Hanne M Boen, Maaike Alaerts, Inge Goovaerts, Johan B Saenen, Constantijn Franssen, Anne Vorlat, Tom Vermeulen, Hein Heidbuchel, Lut Van Laer, Bart Loeys, Emeline M Van Craenenbroeck
{"title":"蒽环类化疗后癌症治疗相关心功能障碍患者的心脏结构基因变异:一项病例对照研究。","authors":"Hanne M Boen, Maaike Alaerts, Inge Goovaerts, Johan B Saenen, Constantijn Franssen, Anne Vorlat, Tom Vermeulen, Hein Heidbuchel, Lut Van Laer, Bart Loeys, Emeline M Van Craenenbroeck","doi":"10.1186/s40959-024-00231-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Variants in cardiomyopathy genes have been identified in patients with cancer therapy-related cardiac dysfunction (CTRCD), suggesting a genetic predisposition for the development of CTRCD. The diagnostic yield of genetic testing in a CTRCD population compared to a cardiomyopathy patient cohort is not yet known and information on which genes should be assessed in this population is lacking.</p><p><strong>Methods: </strong>We retrospectively included 46 cancer patients with a history of anthracycline induced CTRCD (defined as a decrease in left ventricular ejection fraction (LVEF) to < 50% and a ≥ 10% reduction from baseline by echocardiography). Genetic testing was performed for 59 established cardiomyopathy genes. Only variants of uncertain significance and (likely) pathogenic variants were included. Diagnostic yield of genetic testing was compared with a matched cohort of patients with dilated cardiomyopathy (DCM, n = 46) and a matched cohort of patients without cardiac disease (n = 111).</p><p><strong>Results: </strong>Average LVEF at time of CTRCD diagnosis was 30.1 ± 11.0%. Patients were 52.9 ± 14.6 years old at time of diagnosis and 30 (65.2%) were female. Most patients were treated for breast cancer or lymphoma, with a median doxorubicin equivalent dose of 300 mg/m<sup>2</sup> [112.5-540.0]. A genetic variant, either pathogenic, likely pathogenic or of uncertain significance, was identified in 29/46 (63.0%) of patients with CTRCD, which is similar to the DCM cohort (34/46, 73.9%, p = 0.262), but significantly higher than in the negative control cohort (47/111, 39.6%, p = 0.018). Variants in TTN were the most prevalent in the CTRCD cohort (43% of all variants). All (likely) pathogenic variants identified in the CTRCD cohort were truncating variants in TTN. There were no significant differences in severity of CTRCD and in recovery rate in variant-harbouring individuals versus non-variant harbouring individuals.</p><p><strong>Conclusions: </strong>In this case-control study, cancer patients with anthracycline-induced CTRCD have an increased burden of genetic variants in cardiomyopathy genes, similar to a DCM cohort. If validated in larger prospective studies, integration of genetic data in risk prediction models for CTRCD may guide cancer treatment. Moreover, genetic results have important clinical impact, both for the patient in the setting of precision medicine, as for the family members that will receive genetic counselling.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"10 1","pages":"26"},"PeriodicalIF":3.2000,"publicationDate":"2024-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11059765/pdf/","citationCount":"0","resultStr":"{\"title\":\"Variants in structural cardiac genes in patients with cancer therapy-related cardiac dysfunction after anthracycline chemotherapy: a case control study.\",\"authors\":\"Hanne M Boen, Maaike Alaerts, Inge Goovaerts, Johan B Saenen, Constantijn Franssen, Anne Vorlat, Tom Vermeulen, Hein Heidbuchel, Lut Van Laer, Bart Loeys, Emeline M Van Craenenbroeck\",\"doi\":\"10.1186/s40959-024-00231-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Variants in cardiomyopathy genes have been identified in patients with cancer therapy-related cardiac dysfunction (CTRCD), suggesting a genetic predisposition for the development of CTRCD. The diagnostic yield of genetic testing in a CTRCD population compared to a cardiomyopathy patient cohort is not yet known and information on which genes should be assessed in this population is lacking.</p><p><strong>Methods: </strong>We retrospectively included 46 cancer patients with a history of anthracycline induced CTRCD (defined as a decrease in left ventricular ejection fraction (LVEF) to < 50% and a ≥ 10% reduction from baseline by echocardiography). Genetic testing was performed for 59 established cardiomyopathy genes. Only variants of uncertain significance and (likely) pathogenic variants were included. Diagnostic yield of genetic testing was compared with a matched cohort of patients with dilated cardiomyopathy (DCM, n = 46) and a matched cohort of patients without cardiac disease (n = 111).</p><p><strong>Results: </strong>Average LVEF at time of CTRCD diagnosis was 30.1 ± 11.0%. Patients were 52.9 ± 14.6 years old at time of diagnosis and 30 (65.2%) were female. Most patients were treated for breast cancer or lymphoma, with a median doxorubicin equivalent dose of 300 mg/m<sup>2</sup> [112.5-540.0]. A genetic variant, either pathogenic, likely pathogenic or of uncertain significance, was identified in 29/46 (63.0%) of patients with CTRCD, which is similar to the DCM cohort (34/46, 73.9%, p = 0.262), but significantly higher than in the negative control cohort (47/111, 39.6%, p = 0.018). Variants in TTN were the most prevalent in the CTRCD cohort (43% of all variants). All (likely) pathogenic variants identified in the CTRCD cohort were truncating variants in TTN. There were no significant differences in severity of CTRCD and in recovery rate in variant-harbouring individuals versus non-variant harbouring individuals.</p><p><strong>Conclusions: </strong>In this case-control study, cancer patients with anthracycline-induced CTRCD have an increased burden of genetic variants in cardiomyopathy genes, similar to a DCM cohort. If validated in larger prospective studies, integration of genetic data in risk prediction models for CTRCD may guide cancer treatment. Moreover, genetic results have important clinical impact, both for the patient in the setting of precision medicine, as for the family members that will receive genetic counselling.</p>\",\"PeriodicalId\":9804,\"journal\":{\"name\":\"Cardio-oncology\",\"volume\":\"10 1\",\"pages\":\"26\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11059765/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardio-oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-024-00231-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-024-00231-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Variants in structural cardiac genes in patients with cancer therapy-related cardiac dysfunction after anthracycline chemotherapy: a case control study.
Background: Variants in cardiomyopathy genes have been identified in patients with cancer therapy-related cardiac dysfunction (CTRCD), suggesting a genetic predisposition for the development of CTRCD. The diagnostic yield of genetic testing in a CTRCD population compared to a cardiomyopathy patient cohort is not yet known and information on which genes should be assessed in this population is lacking.
Methods: We retrospectively included 46 cancer patients with a history of anthracycline induced CTRCD (defined as a decrease in left ventricular ejection fraction (LVEF) to < 50% and a ≥ 10% reduction from baseline by echocardiography). Genetic testing was performed for 59 established cardiomyopathy genes. Only variants of uncertain significance and (likely) pathogenic variants were included. Diagnostic yield of genetic testing was compared with a matched cohort of patients with dilated cardiomyopathy (DCM, n = 46) and a matched cohort of patients without cardiac disease (n = 111).
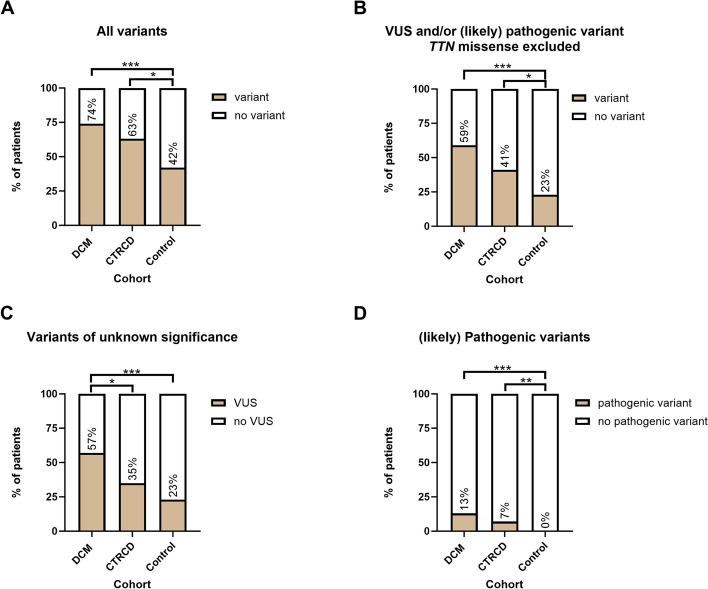
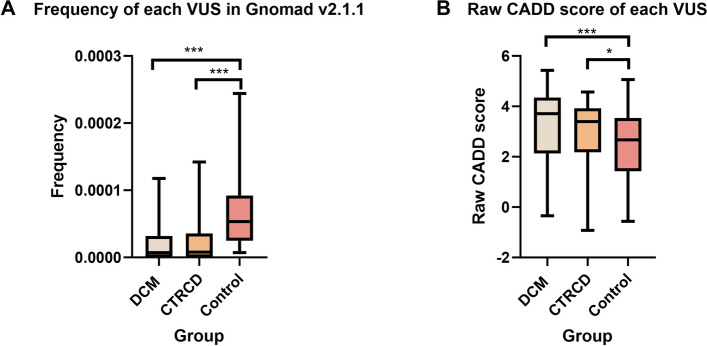
Results: Average LVEF at time of CTRCD diagnosis was 30.1 ± 11.0%. Patients were 52.9 ± 14.6 years old at time of diagnosis and 30 (65.2%) were female. Most patients were treated for breast cancer or lymphoma, with a median doxorubicin equivalent dose of 300 mg/m2 [112.5-540.0]. A genetic variant, either pathogenic, likely pathogenic or of uncertain significance, was identified in 29/46 (63.0%) of patients with CTRCD, which is similar to the DCM cohort (34/46, 73.9%, p = 0.262), but significantly higher than in the negative control cohort (47/111, 39.6%, p = 0.018). Variants in TTN were the most prevalent in the CTRCD cohort (43% of all variants). All (likely) pathogenic variants identified in the CTRCD cohort were truncating variants in TTN. There were no significant differences in severity of CTRCD and in recovery rate in variant-harbouring individuals versus non-variant harbouring individuals.
Conclusions: In this case-control study, cancer patients with anthracycline-induced CTRCD have an increased burden of genetic variants in cardiomyopathy genes, similar to a DCM cohort. If validated in larger prospective studies, integration of genetic data in risk prediction models for CTRCD may guide cancer treatment. Moreover, genetic results have important clinical impact, both for the patient in the setting of precision medicine, as for the family members that will receive genetic counselling.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
