{"title":"使用内窥镜注射针对闭塞的布劳恩吻合口进行内窥镜再通路。","authors":"Hiromune Katsuda, Masanori Kobayashi, Ryuichi Okamoto","doi":"10.1111/den.14814","DOIUrl":null,"url":null,"abstract":"<p>Braun reconstruction is effective in preventing afferent loop syndrome (ALS) after pancreatoduodenectomy.<span><sup>1</sup></span> Occlusion of a Braun anastomosis can lead to ALS, posing a risk of nonobstructive cholangitis.<span><sup>2</sup></span> In such circumstances, surgical reconstruction is highly invasive, and although endoscopic ultrasonography (EUS)-guided enterostomy offers a less invasive alternative,<span><sup>3, 4</sup></span> challenging cases still exist. We hereby report the safer endoscopic recanalization for an occluded Braun anastomosis using an endoscopic needle (Video S1).</p><p>An 83-year-old man, with a history of pancreaticoduodenectomy and Child's reconstruction, developed recurrent cholangitis. Balloon-assisted enteroscopy showed no stenosis at the choledocojejunostomy site, but revealed complete closure of the Braun anastomosis (Fig. 1). To address the potential cause of recurrent cholangitis, an endoscopic attempt was made to recanalize the Braun anastomosis. We discovered that a 20G endoscopic injection needle (Varixer needle (01941); Top, Tokyo, Japan) designed for endoscopic injection sclerotherapy is compatible with a 0.018 inch guidewire (Fielder 18; Olympus, Tokyo, Japan). This needle has a slenderer outer sheath than the EUS-guided fine-needle aspiration needle. Unlike the latter, the metal needle is limited to the tip (Fig. 2a), enabling flexible adaptation to the steep bending angles of the endoscope (Fig. 2b). We aimed for safe recanalization using a rendezvous method, puncturing from the efferent loop to facilitate dilation from the afferent loop, where applying force was more feasible in this case. Despite the endoscope being deeply angulated, the puncture was easily performed, allowing for the placement of a 0.018 inch guidewire (Fig. 2c). As a result, we were able to grasp the guidewire from the afferent loop side, enabling subsequent fistula dilation and stent placement exceptionally easily (Fig. 2d). This technique can be used for the occluded choledocojejunostomy site<span><sup>5</sup></span> and is a valuable method for recanalization of closed intestinal anastomoses.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 7","pages":"851-852"},"PeriodicalIF":3.6000,"publicationDate":"2024-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14814","citationCount":"0","resultStr":"{\"title\":\"Endoscopic recanalization of an occluded Braun anastomosis using an endoscopic injection needle\",\"authors\":\"Hiromune Katsuda, Masanori Kobayashi, Ryuichi Okamoto\",\"doi\":\"10.1111/den.14814\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Braun reconstruction is effective in preventing afferent loop syndrome (ALS) after pancreatoduodenectomy.<span><sup>1</sup></span> Occlusion of a Braun anastomosis can lead to ALS, posing a risk of nonobstructive cholangitis.<span><sup>2</sup></span> In such circumstances, surgical reconstruction is highly invasive, and although endoscopic ultrasonography (EUS)-guided enterostomy offers a less invasive alternative,<span><sup>3, 4</sup></span> challenging cases still exist. We hereby report the safer endoscopic recanalization for an occluded Braun anastomosis using an endoscopic needle (Video S1).</p><p>An 83-year-old man, with a history of pancreaticoduodenectomy and Child's reconstruction, developed recurrent cholangitis. Balloon-assisted enteroscopy showed no stenosis at the choledocojejunostomy site, but revealed complete closure of the Braun anastomosis (Fig. 1). To address the potential cause of recurrent cholangitis, an endoscopic attempt was made to recanalize the Braun anastomosis. We discovered that a 20G endoscopic injection needle (Varixer needle (01941); Top, Tokyo, Japan) designed for endoscopic injection sclerotherapy is compatible with a 0.018 inch guidewire (Fielder 18; Olympus, Tokyo, Japan). This needle has a slenderer outer sheath than the EUS-guided fine-needle aspiration needle. Unlike the latter, the metal needle is limited to the tip (Fig. 2a), enabling flexible adaptation to the steep bending angles of the endoscope (Fig. 2b). We aimed for safe recanalization using a rendezvous method, puncturing from the efferent loop to facilitate dilation from the afferent loop, where applying force was more feasible in this case. Despite the endoscope being deeply angulated, the puncture was easily performed, allowing for the placement of a 0.018 inch guidewire (Fig. 2c). As a result, we were able to grasp the guidewire from the afferent loop side, enabling subsequent fistula dilation and stent placement exceptionally easily (Fig. 2d). This technique can be used for the occluded choledocojejunostomy site<span><sup>5</sup></span> and is a valuable method for recanalization of closed intestinal anastomoses.</p><p>Authors declare no conflict of interest for this article.</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":\"36 7\",\"pages\":\"851-852\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-05-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14814\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14814\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14814","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Endoscopic recanalization of an occluded Braun anastomosis using an endoscopic injection needle
Braun reconstruction is effective in preventing afferent loop syndrome (ALS) after pancreatoduodenectomy.1 Occlusion of a Braun anastomosis can lead to ALS, posing a risk of nonobstructive cholangitis.2 In such circumstances, surgical reconstruction is highly invasive, and although endoscopic ultrasonography (EUS)-guided enterostomy offers a less invasive alternative,3, 4 challenging cases still exist. We hereby report the safer endoscopic recanalization for an occluded Braun anastomosis using an endoscopic needle (Video S1).
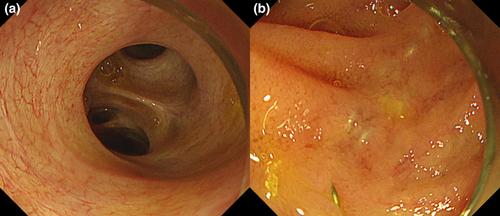
An 83-year-old man, with a history of pancreaticoduodenectomy and Child's reconstruction, developed recurrent cholangitis. Balloon-assisted enteroscopy showed no stenosis at the choledocojejunostomy site, but revealed complete closure of the Braun anastomosis (Fig. 1). To address the potential cause of recurrent cholangitis, an endoscopic attempt was made to recanalize the Braun anastomosis. We discovered that a 20G endoscopic injection needle (Varixer needle (01941); Top, Tokyo, Japan) designed for endoscopic injection sclerotherapy is compatible with a 0.018 inch guidewire (Fielder 18; Olympus, Tokyo, Japan). This needle has a slenderer outer sheath than the EUS-guided fine-needle aspiration needle. Unlike the latter, the metal needle is limited to the tip (Fig. 2a), enabling flexible adaptation to the steep bending angles of the endoscope (Fig. 2b). We aimed for safe recanalization using a rendezvous method, puncturing from the efferent loop to facilitate dilation from the afferent loop, where applying force was more feasible in this case. Despite the endoscope being deeply angulated, the puncture was easily performed, allowing for the placement of a 0.018 inch guidewire (Fig. 2c). As a result, we were able to grasp the guidewire from the afferent loop side, enabling subsequent fistula dilation and stent placement exceptionally easily (Fig. 2d). This technique can be used for the occluded choledocojejunostomy site5 and is a valuable method for recanalization of closed intestinal anastomoses.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
