Daniel Jakob, Valerie Orth, Daniel Gödde, Hubert Zirngibl, Peter C Ambe
{"title":"将家族史作为结直肠癌微卫星不稳定性筛查的主要先决条件,是一种糟糕的选择工具。","authors":"Daniel Jakob, Valerie Orth, Daniel Gödde, Hubert Zirngibl, Peter C Ambe","doi":"10.21037/tgh-23-71","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Deficient mismatch repair (MMR) leading to microsatellite instability (MSI) in tumors is thought to be present in over 15% of colorectal cancer (CRC) cases. Testing CRC for MSI has traditionally been recommended following the fulfillment of clinical criteria. However, the performance of clinical criteria, especially the family history, as a selection tool for MSI screening in CRC is questionable.</p><p><strong>Methods: </strong>We retrospectively investigated the incidence of high degree MSI (MSI-H) tumors in an unselected population of CRC patients and compared its prevalence between individuals with and without family history of cancers within the spectrum of MSI-H tumors as defined in the revised Bethesda criteria.</p><p><strong>Results: </strong>The study population included 274 patients, 70 with positive and 204 without family history of MSI-H tumors with complete data including findings from MSI analysis. The overall incidence of MSI-H CRC was 18.98%. There was no statistically significant difference in the incidence of MSI-H CRC amongst both groups. The sensitivity and specificity of family history with regard to the presence of an MSI-H tumor in this collective was 36.5% and 77.5%, respectively.</p><p><strong>Conclusions: </strong>A relevant number of cases with high MSI-H CRC may be missed secondary to screening based on clinical criteria like family history alone. Thus, systematic screening independent of clinical characteristics, especially family history of cancer should be recommended in all cases with CRC.</p>","PeriodicalId":94362,"journal":{"name":"Translational gastroenterology and hepatology","volume":"9 ","pages":"17"},"PeriodicalIF":2.5000,"publicationDate":"2024-03-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11074476/pdf/","citationCount":"0","resultStr":"{\"title\":\"Family history as a major prerequisite for microsatellite instability screening in colorectal cancer is a poor selection tool.\",\"authors\":\"Daniel Jakob, Valerie Orth, Daniel Gödde, Hubert Zirngibl, Peter C Ambe\",\"doi\":\"10.21037/tgh-23-71\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Deficient mismatch repair (MMR) leading to microsatellite instability (MSI) in tumors is thought to be present in over 15% of colorectal cancer (CRC) cases. Testing CRC for MSI has traditionally been recommended following the fulfillment of clinical criteria. However, the performance of clinical criteria, especially the family history, as a selection tool for MSI screening in CRC is questionable.</p><p><strong>Methods: </strong>We retrospectively investigated the incidence of high degree MSI (MSI-H) tumors in an unselected population of CRC patients and compared its prevalence between individuals with and without family history of cancers within the spectrum of MSI-H tumors as defined in the revised Bethesda criteria.</p><p><strong>Results: </strong>The study population included 274 patients, 70 with positive and 204 without family history of MSI-H tumors with complete data including findings from MSI analysis. The overall incidence of MSI-H CRC was 18.98%. There was no statistically significant difference in the incidence of MSI-H CRC amongst both groups. The sensitivity and specificity of family history with regard to the presence of an MSI-H tumor in this collective was 36.5% and 77.5%, respectively.</p><p><strong>Conclusions: </strong>A relevant number of cases with high MSI-H CRC may be missed secondary to screening based on clinical criteria like family history alone. Thus, systematic screening independent of clinical characteristics, especially family history of cancer should be recommended in all cases with CRC.</p>\",\"PeriodicalId\":94362,\"journal\":{\"name\":\"Translational gastroenterology and hepatology\",\"volume\":\"9 \",\"pages\":\"17\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-03-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11074476/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational gastroenterology and hepatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/tgh-23-71\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/tgh-23-71","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Family history as a major prerequisite for microsatellite instability screening in colorectal cancer is a poor selection tool.
Background: Deficient mismatch repair (MMR) leading to microsatellite instability (MSI) in tumors is thought to be present in over 15% of colorectal cancer (CRC) cases. Testing CRC for MSI has traditionally been recommended following the fulfillment of clinical criteria. However, the performance of clinical criteria, especially the family history, as a selection tool for MSI screening in CRC is questionable.
Methods: We retrospectively investigated the incidence of high degree MSI (MSI-H) tumors in an unselected population of CRC patients and compared its prevalence between individuals with and without family history of cancers within the spectrum of MSI-H tumors as defined in the revised Bethesda criteria.
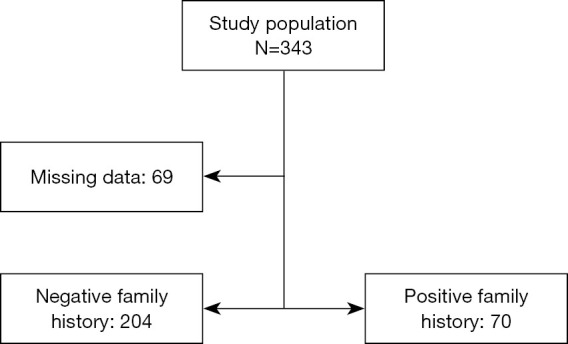
Results: The study population included 274 patients, 70 with positive and 204 without family history of MSI-H tumors with complete data including findings from MSI analysis. The overall incidence of MSI-H CRC was 18.98%. There was no statistically significant difference in the incidence of MSI-H CRC amongst both groups. The sensitivity and specificity of family history with regard to the presence of an MSI-H tumor in this collective was 36.5% and 77.5%, respectively.
Conclusions: A relevant number of cases with high MSI-H CRC may be missed secondary to screening based on clinical criteria like family history alone. Thus, systematic screening independent of clinical characteristics, especially family history of cancer should be recommended in all cases with CRC.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
