{"title":"临床与实验过敏》杂志的快速临床试验评估。","authors":"Robert J. Boyle, Mohamed H. Shamji","doi":"10.1111/cea.14492","DOIUrl":null,"url":null,"abstract":"<p>This month the editors of Clinical and Experimental Allergy are pleased to announce a new Fast Track editorial process for Clinical Trials. We are keen to encourage submissions of Clinical Trial manuscripts to the journal, and are therefore offering accelerated editorial decision-making and peer review when authors request this service (Table 1). To submit an article for Fast Track assessment, we encourage early communication with the Editors in Chief so that we can plan for receipt of the manuscript. Fast Track assessment will be able to be requested during the online submission process, for manuscripts classified as a Clinical Trial. Authors of Clinical Trial manuscripts who do not choose Fast Track will still have their manuscripts reviewed by an editor but without these accelerated timelines. Clinical Trials form the bedrock of evidence for the efficacy and safety of interventions in healthcare and public health. While clinical trial populations are not always representative of more general populations where an intervention might be applied, the process of randomisation is key to reducing risk of confounding, which besets many types of observational studies. Despite decades of pressure from academics, patient groups, charities and governments, transparency in clinical trials is still an ongoing issue, leading to bias in the availability of trial results. Many clinical trials are still not registered prior to inception, remain unpublished following completion or selectively report their findings.<span><sup>1</sup></span> At Clinical and Experimental Allergy, we are committed to transparent and complete reporting of clinical trial findings, so that the scientific community, healthcare professionals, policy-makers and the public can learn as much as possible from each completed trial.</p><p>Summary of accelerated timeline for Fast Track Clinical Trial submissions to Clinical and Experimental Allergy from May 2024 onwards. * Editorial decision means the decision by an Editor to reject the manuscript or send the manuscript for peer review. First decision means the decision by an Editor to reject, accept or request revisions for a manuscript.</p><p>In this issue of the journal, we highlight two clinical trial reports. The first is a protocol for a randomised, controlled feasibility trial of an intervention designed to influence bathing frequency during infancy, something that may be relevant to the early development of eczema or food allergies.<span><sup>2</sup></span> The BabyBathe trial is summarised in Figure 1, and is an example of transparent a priori reporting of clinical trial plans. The trial was registered prior to enrolment of the first participant at a World Health Organization approved clinical trials registry, and authors have followed best practice by sharing full details of their intervention development process and the participant information and consent form for enrolment in the BabyBathe trial. Public availability of the participant information and consent form means that assessors can try to evaluate the degree of equipoise in investigators and participants at enrolment, something that is especially important in trials where outcomes are recorded or reported by people who are aware of the treatment allocation. If participants are advised that an intervention is exciting and likely to have favourable health effects, and they are aware of their treatment allocation, then their reporting of health effects of the intervention may be prone to bias. In contrast, a participant information sheet that reflects equipoise and uncertainty about the health effects of the intervention may be less prone to this form of outcome reporting bias. Registered protocols and participant information sheets with equipoise do not guarantee an absence of outcome reporting bias, which can take many forms, but making the protocol and information sheet publicly available are simple steps which help to improve transparency.<span><sup>3</sup></span></p><p>A second clinical trial publication in this month's issue is a completed randomised controlled trial.<span><sup>4</sup></span> In this case, the trial is industry-sponsored and the analysis focuses on a <i>post hoc</i> assessment, suggesting the company's product may have positive health impacts on patients with asthma. Again, this clinical trial was registered in a World Health Organization approved clinical trials registry and authors have made the pre-trial clinical trial protocol available on a publicly accessible website, which can be linked to from the clinical trial report in this issue. For transparency, the <i>post hoc</i> nature of the favourable analysis, and the source of study funding, are both clearly indicated in the article.</p><p>While clinical trials form the bedrock of evidence for interventions in healthcare and public health, they often need to be synthesised and summarised for end-users to make sense of what the trials are telling us about intervention effects. This is typically undertaken as a systematic review, a methodology that has proliferated since the inception of the Cochrane Collaboration 30 years ago. Most guideline development groups now rely on systematic reviews of clinical trials and other forms of evidence to support their decision-making while developing practice guidelines. We aim to publish a summary of a recent, allergy-relevant Cochrane review in every issue of Clinical and Experimental Allergy. This month's Cochrane Corner summarises evidence for psychological interventions in children and young people with asthma.<span><sup>5</sup></span> Asthma is associated with increased anxiety, partly due to the intermittent experience of breathlessness and associated impact on daily activities. Anxiety is amenable to psychological therapies, so it makes sense that this type of treatment may have benefits for some children and young people with asthma. In the recent Cochrane Review of this topic, authors found some evidence to support positive health effects in this population, but there were significant limitations. As with so many Cochrane reviews, authors noted issues related to selective reporting bias and heterogeneity, and so judged the certainty of evidence as low. Currently, there is evidence to support using psychological therapies to help with associated anxiety or depression in young people with asthma, but there is insufficient evidence to support favourable effects on respiratory outcomes.</p><p>RJB drafted the manuscript. MHS approved the manuscript.</p><p>Both authors declare no conflict of interest in relation to this article.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 5","pages":"308-310"},"PeriodicalIF":5.2000,"publicationDate":"2024-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14492","citationCount":"0","resultStr":"{\"title\":\"Fast Track Clinical Trials assessment at Clinical & Experimental Allergy\",\"authors\":\"Robert J. Boyle, Mohamed H. Shamji\",\"doi\":\"10.1111/cea.14492\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>This month the editors of Clinical and Experimental Allergy are pleased to announce a new Fast Track editorial process for Clinical Trials. We are keen to encourage submissions of Clinical Trial manuscripts to the journal, and are therefore offering accelerated editorial decision-making and peer review when authors request this service (Table 1). To submit an article for Fast Track assessment, we encourage early communication with the Editors in Chief so that we can plan for receipt of the manuscript. Fast Track assessment will be able to be requested during the online submission process, for manuscripts classified as a Clinical Trial. Authors of Clinical Trial manuscripts who do not choose Fast Track will still have their manuscripts reviewed by an editor but without these accelerated timelines. Clinical Trials form the bedrock of evidence for the efficacy and safety of interventions in healthcare and public health. While clinical trial populations are not always representative of more general populations where an intervention might be applied, the process of randomisation is key to reducing risk of confounding, which besets many types of observational studies. Despite decades of pressure from academics, patient groups, charities and governments, transparency in clinical trials is still an ongoing issue, leading to bias in the availability of trial results. Many clinical trials are still not registered prior to inception, remain unpublished following completion or selectively report their findings.<span><sup>1</sup></span> At Clinical and Experimental Allergy, we are committed to transparent and complete reporting of clinical trial findings, so that the scientific community, healthcare professionals, policy-makers and the public can learn as much as possible from each completed trial.</p><p>Summary of accelerated timeline for Fast Track Clinical Trial submissions to Clinical and Experimental Allergy from May 2024 onwards. * Editorial decision means the decision by an Editor to reject the manuscript or send the manuscript for peer review. First decision means the decision by an Editor to reject, accept or request revisions for a manuscript.</p><p>In this issue of the journal, we highlight two clinical trial reports. The first is a protocol for a randomised, controlled feasibility trial of an intervention designed to influence bathing frequency during infancy, something that may be relevant to the early development of eczema or food allergies.<span><sup>2</sup></span> The BabyBathe trial is summarised in Figure 1, and is an example of transparent a priori reporting of clinical trial plans. The trial was registered prior to enrolment of the first participant at a World Health Organization approved clinical trials registry, and authors have followed best practice by sharing full details of their intervention development process and the participant information and consent form for enrolment in the BabyBathe trial. Public availability of the participant information and consent form means that assessors can try to evaluate the degree of equipoise in investigators and participants at enrolment, something that is especially important in trials where outcomes are recorded or reported by people who are aware of the treatment allocation. If participants are advised that an intervention is exciting and likely to have favourable health effects, and they are aware of their treatment allocation, then their reporting of health effects of the intervention may be prone to bias. In contrast, a participant information sheet that reflects equipoise and uncertainty about the health effects of the intervention may be less prone to this form of outcome reporting bias. Registered protocols and participant information sheets with equipoise do not guarantee an absence of outcome reporting bias, which can take many forms, but making the protocol and information sheet publicly available are simple steps which help to improve transparency.<span><sup>3</sup></span></p><p>A second clinical trial publication in this month's issue is a completed randomised controlled trial.<span><sup>4</sup></span> In this case, the trial is industry-sponsored and the analysis focuses on a <i>post hoc</i> assessment, suggesting the company's product may have positive health impacts on patients with asthma. Again, this clinical trial was registered in a World Health Organization approved clinical trials registry and authors have made the pre-trial clinical trial protocol available on a publicly accessible website, which can be linked to from the clinical trial report in this issue. For transparency, the <i>post hoc</i> nature of the favourable analysis, and the source of study funding, are both clearly indicated in the article.</p><p>While clinical trials form the bedrock of evidence for interventions in healthcare and public health, they often need to be synthesised and summarised for end-users to make sense of what the trials are telling us about intervention effects. This is typically undertaken as a systematic review, a methodology that has proliferated since the inception of the Cochrane Collaboration 30 years ago. Most guideline development groups now rely on systematic reviews of clinical trials and other forms of evidence to support their decision-making while developing practice guidelines. We aim to publish a summary of a recent, allergy-relevant Cochrane review in every issue of Clinical and Experimental Allergy. This month's Cochrane Corner summarises evidence for psychological interventions in children and young people with asthma.<span><sup>5</sup></span> Asthma is associated with increased anxiety, partly due to the intermittent experience of breathlessness and associated impact on daily activities. Anxiety is amenable to psychological therapies, so it makes sense that this type of treatment may have benefits for some children and young people with asthma. In the recent Cochrane Review of this topic, authors found some evidence to support positive health effects in this population, but there were significant limitations. As with so many Cochrane reviews, authors noted issues related to selective reporting bias and heterogeneity, and so judged the certainty of evidence as low. Currently, there is evidence to support using psychological therapies to help with associated anxiety or depression in young people with asthma, but there is insufficient evidence to support favourable effects on respiratory outcomes.</p><p>RJB drafted the manuscript. MHS approved the manuscript.</p><p>Both authors declare no conflict of interest in relation to this article.</p>\",\"PeriodicalId\":10207,\"journal\":{\"name\":\"Clinical and Experimental Allergy\",\"volume\":\"54 5\",\"pages\":\"308-310\"},\"PeriodicalIF\":5.2000,\"publicationDate\":\"2024-05-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14492\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cea.14492\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14492","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
Fast Track Clinical Trials assessment at Clinical & Experimental Allergy
This month the editors of Clinical and Experimental Allergy are pleased to announce a new Fast Track editorial process for Clinical Trials. We are keen to encourage submissions of Clinical Trial manuscripts to the journal, and are therefore offering accelerated editorial decision-making and peer review when authors request this service (Table 1). To submit an article for Fast Track assessment, we encourage early communication with the Editors in Chief so that we can plan for receipt of the manuscript. Fast Track assessment will be able to be requested during the online submission process, for manuscripts classified as a Clinical Trial. Authors of Clinical Trial manuscripts who do not choose Fast Track will still have their manuscripts reviewed by an editor but without these accelerated timelines. Clinical Trials form the bedrock of evidence for the efficacy and safety of interventions in healthcare and public health. While clinical trial populations are not always representative of more general populations where an intervention might be applied, the process of randomisation is key to reducing risk of confounding, which besets many types of observational studies. Despite decades of pressure from academics, patient groups, charities and governments, transparency in clinical trials is still an ongoing issue, leading to bias in the availability of trial results. Many clinical trials are still not registered prior to inception, remain unpublished following completion or selectively report their findings.1 At Clinical and Experimental Allergy, we are committed to transparent and complete reporting of clinical trial findings, so that the scientific community, healthcare professionals, policy-makers and the public can learn as much as possible from each completed trial.
Summary of accelerated timeline for Fast Track Clinical Trial submissions to Clinical and Experimental Allergy from May 2024 onwards. * Editorial decision means the decision by an Editor to reject the manuscript or send the manuscript for peer review. First decision means the decision by an Editor to reject, accept or request revisions for a manuscript.
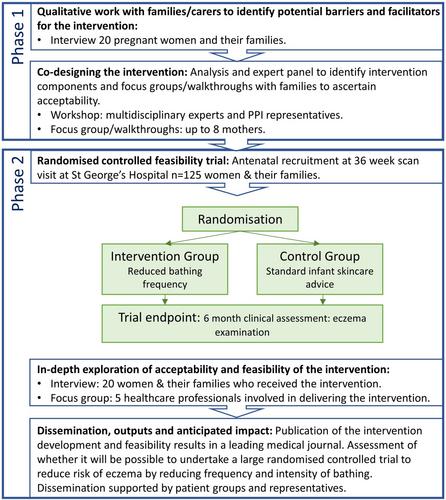
In this issue of the journal, we highlight two clinical trial reports. The first is a protocol for a randomised, controlled feasibility trial of an intervention designed to influence bathing frequency during infancy, something that may be relevant to the early development of eczema or food allergies.2 The BabyBathe trial is summarised in Figure 1, and is an example of transparent a priori reporting of clinical trial plans. The trial was registered prior to enrolment of the first participant at a World Health Organization approved clinical trials registry, and authors have followed best practice by sharing full details of their intervention development process and the participant information and consent form for enrolment in the BabyBathe trial. Public availability of the participant information and consent form means that assessors can try to evaluate the degree of equipoise in investigators and participants at enrolment, something that is especially important in trials where outcomes are recorded or reported by people who are aware of the treatment allocation. If participants are advised that an intervention is exciting and likely to have favourable health effects, and they are aware of their treatment allocation, then their reporting of health effects of the intervention may be prone to bias. In contrast, a participant information sheet that reflects equipoise and uncertainty about the health effects of the intervention may be less prone to this form of outcome reporting bias. Registered protocols and participant information sheets with equipoise do not guarantee an absence of outcome reporting bias, which can take many forms, but making the protocol and information sheet publicly available are simple steps which help to improve transparency.3
A second clinical trial publication in this month's issue is a completed randomised controlled trial.4 In this case, the trial is industry-sponsored and the analysis focuses on a post hoc assessment, suggesting the company's product may have positive health impacts on patients with asthma. Again, this clinical trial was registered in a World Health Organization approved clinical trials registry and authors have made the pre-trial clinical trial protocol available on a publicly accessible website, which can be linked to from the clinical trial report in this issue. For transparency, the post hoc nature of the favourable analysis, and the source of study funding, are both clearly indicated in the article.
While clinical trials form the bedrock of evidence for interventions in healthcare and public health, they often need to be synthesised and summarised for end-users to make sense of what the trials are telling us about intervention effects. This is typically undertaken as a systematic review, a methodology that has proliferated since the inception of the Cochrane Collaboration 30 years ago. Most guideline development groups now rely on systematic reviews of clinical trials and other forms of evidence to support their decision-making while developing practice guidelines. We aim to publish a summary of a recent, allergy-relevant Cochrane review in every issue of Clinical and Experimental Allergy. This month's Cochrane Corner summarises evidence for psychological interventions in children and young people with asthma.5 Asthma is associated with increased anxiety, partly due to the intermittent experience of breathlessness and associated impact on daily activities. Anxiety is amenable to psychological therapies, so it makes sense that this type of treatment may have benefits for some children and young people with asthma. In the recent Cochrane Review of this topic, authors found some evidence to support positive health effects in this population, but there were significant limitations. As with so many Cochrane reviews, authors noted issues related to selective reporting bias and heterogeneity, and so judged the certainty of evidence as low. Currently, there is evidence to support using psychological therapies to help with associated anxiety or depression in young people with asthma, but there is insufficient evidence to support favourable effects on respiratory outcomes.
RJB drafted the manuscript. MHS approved the manuscript.
Both authors declare no conflict of interest in relation to this article.
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
