{"title":"用肌层抓取和牵拉技术缝合大肠内镜黏膜下剥离术的黏膜缺损。","authors":"Keisaku Yamada, Masahiro Tajika, Yasumasa Niwa","doi":"10.1111/den.14817","DOIUrl":null,"url":null,"abstract":"<p>In recent years, several suturing methods have been invented to prevent the adverse event of endoscopic submucosal dissection (ESD) such as delayed bleeding.<span><sup>1</sup></span></p><p>Furthermore, it is important to close the entire muscle layer without dead space for a strong suture.<span><sup>2, 3</sup></span></p><p>A 67-year-old female patient presented with a 30 mm 0-IIa lesion in the cecum, and underwent ESD (Video S1).</p><p>First, ESD was performed using an ORISE Proknife (Boston Scientific, Marlborough, MA, USA) from the anal side and en bloc resection was completed. After en bloc resection, a mucosal defect of ~5 cm was observed (Fig. 1), and suturing was performed. First, a clip with nylon thread was attached to the middle of the mucosal defect. The thread was then gently pulled to elevate the grasped muscle layers, while suturing it with a reopenable clip (SureClip; MicroTech, Nanjing, China). In this process, the clip was applied to the submucosal layer at the edge of the mucosal defect, not the mucosa, and sutured to the submucosal layer at the opposite edge along with the elevated muscle layer. The other area was sutured in the same way with a clip by pulling the thread. Once the mucosa on both sides has closed to some extent, additional clips were used to suture the mucosa tightly. Finally, the thread was cut and complete suture was possible (Fig. 2).</p><p>This suturing technique allows the mucosal defect to be reduced by clipping the middle region of the muscle layer. In addition, by hooking the clip not to the mucosa but to the submucosa at the edge of the mucosal defect, the clip is less likely to slip, and by pulling the thread to elevate the muscle layer, the middle muscle layer can be sutured together with both sides, eliminating dead space. This suturing technique is useful for mucosal defect of colorectal ESD.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 7","pages":"853-854"},"PeriodicalIF":5.0000,"publicationDate":"2024-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14817","citationCount":"0","resultStr":"{\"title\":\"Suturing with muscle layer grasping and pulling technique for mucosal defect of colorectal endoscopic submucosal dissection\",\"authors\":\"Keisaku Yamada, Masahiro Tajika, Yasumasa Niwa\",\"doi\":\"10.1111/den.14817\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In recent years, several suturing methods have been invented to prevent the adverse event of endoscopic submucosal dissection (ESD) such as delayed bleeding.<span><sup>1</sup></span></p><p>Furthermore, it is important to close the entire muscle layer without dead space for a strong suture.<span><sup>2, 3</sup></span></p><p>A 67-year-old female patient presented with a 30 mm 0-IIa lesion in the cecum, and underwent ESD (Video S1).</p><p>First, ESD was performed using an ORISE Proknife (Boston Scientific, Marlborough, MA, USA) from the anal side and en bloc resection was completed. After en bloc resection, a mucosal defect of ~5 cm was observed (Fig. 1), and suturing was performed. First, a clip with nylon thread was attached to the middle of the mucosal defect. The thread was then gently pulled to elevate the grasped muscle layers, while suturing it with a reopenable clip (SureClip; MicroTech, Nanjing, China). In this process, the clip was applied to the submucosal layer at the edge of the mucosal defect, not the mucosa, and sutured to the submucosal layer at the opposite edge along with the elevated muscle layer. The other area was sutured in the same way with a clip by pulling the thread. Once the mucosa on both sides has closed to some extent, additional clips were used to suture the mucosa tightly. Finally, the thread was cut and complete suture was possible (Fig. 2).</p><p>This suturing technique allows the mucosal defect to be reduced by clipping the middle region of the muscle layer. In addition, by hooking the clip not to the mucosa but to the submucosa at the edge of the mucosal defect, the clip is less likely to slip, and by pulling the thread to elevate the muscle layer, the middle muscle layer can be sutured together with both sides, eliminating dead space. This suturing technique is useful for mucosal defect of colorectal ESD.</p><p>Authors declare no conflict of interest for this article.</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":\"36 7\",\"pages\":\"853-854\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-05-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14817\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14817\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14817","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Suturing with muscle layer grasping and pulling technique for mucosal defect of colorectal endoscopic submucosal dissection
In recent years, several suturing methods have been invented to prevent the adverse event of endoscopic submucosal dissection (ESD) such as delayed bleeding.1
Furthermore, it is important to close the entire muscle layer without dead space for a strong suture.2, 3
A 67-year-old female patient presented with a 30 mm 0-IIa lesion in the cecum, and underwent ESD (Video S1).
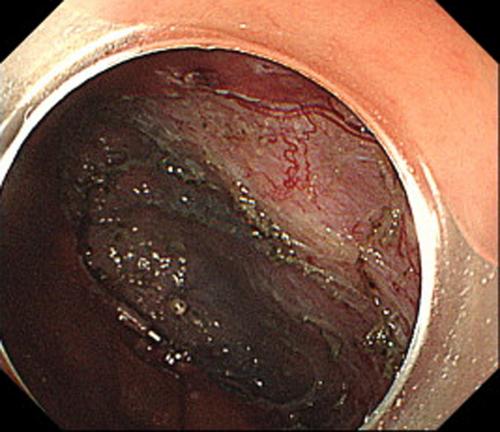
First, ESD was performed using an ORISE Proknife (Boston Scientific, Marlborough, MA, USA) from the anal side and en bloc resection was completed. After en bloc resection, a mucosal defect of ~5 cm was observed (Fig. 1), and suturing was performed. First, a clip with nylon thread was attached to the middle of the mucosal defect. The thread was then gently pulled to elevate the grasped muscle layers, while suturing it with a reopenable clip (SureClip; MicroTech, Nanjing, China). In this process, the clip was applied to the submucosal layer at the edge of the mucosal defect, not the mucosa, and sutured to the submucosal layer at the opposite edge along with the elevated muscle layer. The other area was sutured in the same way with a clip by pulling the thread. Once the mucosa on both sides has closed to some extent, additional clips were used to suture the mucosa tightly. Finally, the thread was cut and complete suture was possible (Fig. 2).
This suturing technique allows the mucosal defect to be reduced by clipping the middle region of the muscle layer. In addition, by hooking the clip not to the mucosa but to the submucosa at the edge of the mucosal defect, the clip is less likely to slip, and by pulling the thread to elevate the muscle layer, the middle muscle layer can be sutured together with both sides, eliminating dead space. This suturing technique is useful for mucosal defect of colorectal ESD.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
