Carlos Diaz-Arocutipa MD, Guillermo Moreno PhD, Lourdes Vicent MD
{"title":"根据虚弱风险对感染性心内膜炎患者进行瓣膜手术的影响。","authors":"Carlos Diaz-Arocutipa MD, Guillermo Moreno PhD, Lourdes Vicent MD","doi":"10.1002/clc.24268","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Observational studies suggest that valvular surgery can reduce mortality in selected patients with infective endocarditis (IE). However, the benefit of this intervention according to frailty levels remains unclear. Our study aims to assess the effect of valvular surgery according to frailty status in this population.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We performed a retrospective study using the 2016−2019 National Inpatient Sample database. Adult patients with a primary diagnosis of IE were included. Frailty was assessed using the Hospital Frailty Risk Score. Inverse probability of treatment weighting (IPTW) was used to balance baseline differences between groups.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 53,275 patients with IE were included, with 18.3% underwent valvular surgery. The median age was 52 (34−68) years, with 41% females. Overall, 42.7% had low risk of frailty, 53.1% intermediate risk, and 4.2% high risk. After IPTW adjustment, in-hospital mortality was similar both for the entire cohort between valvular and non-valvular surgery groups (3.7% vs. 4.1%, <i>p</i> = .483), and low (1% vs. 0.9%, <i>p</i> = .952) or moderate (5.4% vs. 6%, <i>p</i> = .548) risk of frailty. However, patients at high risk of frailty had significantly lower in-hospital mortality in the valvular surgery group (4.6% vs. 13.9%, <i>p</i> = .016). Renal replacement therapy was similar between groups across frailty status. In contrast, surgery was associated with increased use of mechanical circulatory support and pacemaker implantation.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Our findings suggest that there was no difference in survival between valve surgery and medical management in patients at low/intermediate frailty risk, but not for high-risk individuals.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 5","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24268","citationCount":"0","resultStr":"{\"title\":\"Impact of valvular surgery according to frailty risk in patients with infective endocarditis\",\"authors\":\"Carlos Diaz-Arocutipa MD, Guillermo Moreno PhD, Lourdes Vicent MD\",\"doi\":\"10.1002/clc.24268\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Observational studies suggest that valvular surgery can reduce mortality in selected patients with infective endocarditis (IE). However, the benefit of this intervention according to frailty levels remains unclear. Our study aims to assess the effect of valvular surgery according to frailty status in this population.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We performed a retrospective study using the 2016−2019 National Inpatient Sample database. Adult patients with a primary diagnosis of IE were included. Frailty was assessed using the Hospital Frailty Risk Score. Inverse probability of treatment weighting (IPTW) was used to balance baseline differences between groups.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 53,275 patients with IE were included, with 18.3% underwent valvular surgery. The median age was 52 (34−68) years, with 41% females. Overall, 42.7% had low risk of frailty, 53.1% intermediate risk, and 4.2% high risk. After IPTW adjustment, in-hospital mortality was similar both for the entire cohort between valvular and non-valvular surgery groups (3.7% vs. 4.1%, <i>p</i> = .483), and low (1% vs. 0.9%, <i>p</i> = .952) or moderate (5.4% vs. 6%, <i>p</i> = .548) risk of frailty. However, patients at high risk of frailty had significantly lower in-hospital mortality in the valvular surgery group (4.6% vs. 13.9%, <i>p</i> = .016). Renal replacement therapy was similar between groups across frailty status. In contrast, surgery was associated with increased use of mechanical circulatory support and pacemaker implantation.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Our findings suggest that there was no difference in survival between valve surgery and medical management in patients at low/intermediate frailty risk, but not for high-risk individuals.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10201,\"journal\":{\"name\":\"Clinical Cardiology\",\"volume\":\"47 5\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-05-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24268\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.24268\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.24268","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:观察性研究表明,瓣膜手术可降低特定感染性心内膜炎(IE)患者的死亡率。然而,根据虚弱程度进行干预的益处仍不明确。我们的研究旨在根据该人群的虚弱状况评估瓣膜手术的效果:我们利用 2016-2019 年全国住院患者抽样数据库进行了一项回顾性研究。研究纳入了主要诊断为 IE 的成人患者。采用医院虚弱风险评分对患者的虚弱程度进行评估。采用逆概率治疗加权法(IPTW)平衡各组间的基线差异:共纳入了 53275 名 IE 患者,其中 18.3% 接受了瓣膜手术。中位年龄为 52(34-68)岁,女性占 41%。总体而言,42.7%的患者体弱风险较低,53.1%为中度风险,4.2%为高度风险。经过IPTW调整后,整个队列中瓣膜手术组和非瓣膜手术组的院内死亡率相似(3.7% vs. 4.1%,p = .483),虚弱风险为低度(1% vs. 0.9%,p = .952)或中度(5.4% vs. 6%,p = .548)。然而,在瓣膜手术组中,虚弱高风险患者的院内死亡率明显较低(4.6% vs. 13.9%,p = .016)。肾脏替代治疗在不同体弱状况的组别中效果相似。相比之下,手术与机械循环支持和起搏器植入的使用增加有关:我们的研究结果表明,瓣膜手术和内科治疗在低/中度虚弱风险患者的生存率上没有差异,但在高风险患者中则没有差异。
Impact of valvular surgery according to frailty risk in patients with infective endocarditis
Background
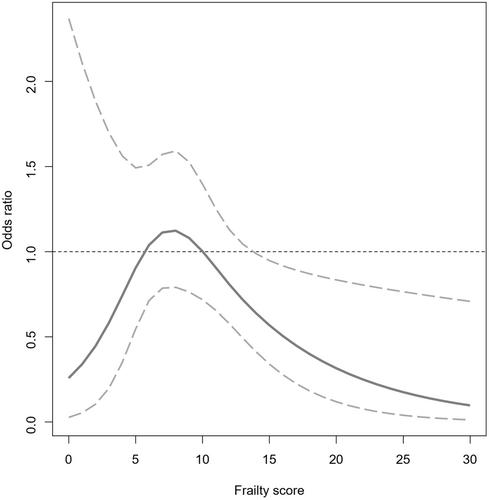
Observational studies suggest that valvular surgery can reduce mortality in selected patients with infective endocarditis (IE). However, the benefit of this intervention according to frailty levels remains unclear. Our study aims to assess the effect of valvular surgery according to frailty status in this population.
Methods
We performed a retrospective study using the 2016−2019 National Inpatient Sample database. Adult patients with a primary diagnosis of IE were included. Frailty was assessed using the Hospital Frailty Risk Score. Inverse probability of treatment weighting (IPTW) was used to balance baseline differences between groups.
Results
A total of 53,275 patients with IE were included, with 18.3% underwent valvular surgery. The median age was 52 (34−68) years, with 41% females. Overall, 42.7% had low risk of frailty, 53.1% intermediate risk, and 4.2% high risk. After IPTW adjustment, in-hospital mortality was similar both for the entire cohort between valvular and non-valvular surgery groups (3.7% vs. 4.1%, p = .483), and low (1% vs. 0.9%, p = .952) or moderate (5.4% vs. 6%, p = .548) risk of frailty. However, patients at high risk of frailty had significantly lower in-hospital mortality in the valvular surgery group (4.6% vs. 13.9%, p = .016). Renal replacement therapy was similar between groups across frailty status. In contrast, surgery was associated with increased use of mechanical circulatory support and pacemaker implantation.
Conclusions
Our findings suggest that there was no difference in survival between valve surgery and medical management in patients at low/intermediate frailty risk, but not for high-risk individuals.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
