Abdulrahman Asiri, Farhan Zayed Alenezi, Hani Tamim, Musharaf Sadat, Felwa Bin Humaid, Wedyan AlWehaibi, Hasan M Al-Dorzi, Yasir Adnan Alzoubi, Samiyah Alrawey Alanazi, Brintha Naidu, Yaseen M Arabi
{"title":"沙特阿拉伯一家三级医院重症监护病房的 \"拒绝复苏令 \"实践和预测因素。","authors":"Abdulrahman Asiri, Farhan Zayed Alenezi, Hani Tamim, Musharaf Sadat, Felwa Bin Humaid, Wedyan AlWehaibi, Hasan M Al-Dorzi, Yasir Adnan Alzoubi, Samiyah Alrawey Alanazi, Brintha Naidu, Yaseen M Arabi","doi":"10.1155/2024/5516516","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The objective of this study was to describe Do-Not-Resuscitate (DNR) practices in a tertiary-care intensive care unit (ICU) in Saudi Arabia, and determine the predictors and outcomes of patients who had DNR orders.</p><p><strong>Methods: </strong>This retrospective cohort study was based on a prospectively collected database for a medical-surgicalIntensive CareDepartment in a tertiary-care center in Riyadh, Saudi Arabia (1999-2017). We compared patients who had DNR orders during the ICU stay with those with \"full code.\" The primary outcome was hospital mortality. The secondary outcomes included ICU mortality, tracheostomy, duration of mechanical ventilation, and length of stay in the ICU and hospital.</p><p><strong>Results: </strong>Among 24790 patients admitted to the ICU over the 19-year study period, 3217 (13%) had DNR orders during the ICU stay. Compared to patients with \"full code,\" patients with DNR orders were older (median 67 years [Q1, Q3: 55, 76] versus 57 years [Q1, Q3: 33, 71], <i>p</i> < 0.0001), were more likely to be females (43% versus 38%, <i>p</i> < 0.0001), had worse premorbid functional status (WHO performance status scores 4-5: 606[18.9%] versus 1894[8.8%], <i>p</i> < 0.0001), higher prevalence of comorbid conditions, and higher APACHE II score (median 28 [Q1, Q3: 23, 34] versus 19 [Q1, Q3: 13, 25], <i>p</i> < 0.0001) and were more likely to be mechanically ventilated (83% versus 55%, <i>p</i> < 0.0001). Patients had DNR orders were more likely to die in the ICU (67.8% versus 8.5%, <i>p</i> < 0.0001) and hospital (82.4% versus 18.1%, <i>p</i> < 0.0001). On multivariable logistic regression analysis, the following were associated with an increased likelihood of DNR status: increasing age (odds ratio (OR) 1.01, 95% confidence interval (CI) 1.01-1.02), higher APACHE II score (OR 1.09, 95% CI 1.08-1.10), and worse WHO performance status score. Patients admitted in recent years (2012-2017 versus 2002-2005) were less likely to have DNR orders (OR 0.35, 95% CI 0.32-0.39, <i>p</i> < 0.0001). Patients with DNR orders had higher ICU mortality, more tracheostomies, longer duration of mechanical ventilation and length of ICU stay compared to patients with with \"full code\" but they had shorter length of hospital stay.</p><p><strong>Conclusion: </strong>In a tertiary-care hospital in Saudi Arabia, 13% of critically ill patients had DNR orders during ICU stay. This study identified several predictors of DNR orders, including the severity of illness and poor premorbid functional status.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2024 ","pages":"5516516"},"PeriodicalIF":1.8000,"publicationDate":"2024-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11090671/pdf/","citationCount":"0","resultStr":"{\"title\":\"Practice and Predictors of Do-Not-Resuscitate Orders in a Tertiary-Care Intensive Care Unit in Saudi Arabia.\",\"authors\":\"Abdulrahman Asiri, Farhan Zayed Alenezi, Hani Tamim, Musharaf Sadat, Felwa Bin Humaid, Wedyan AlWehaibi, Hasan M Al-Dorzi, Yasir Adnan Alzoubi, Samiyah Alrawey Alanazi, Brintha Naidu, Yaseen M Arabi\",\"doi\":\"10.1155/2024/5516516\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The objective of this study was to describe Do-Not-Resuscitate (DNR) practices in a tertiary-care intensive care unit (ICU) in Saudi Arabia, and determine the predictors and outcomes of patients who had DNR orders.</p><p><strong>Methods: </strong>This retrospective cohort study was based on a prospectively collected database for a medical-surgicalIntensive CareDepartment in a tertiary-care center in Riyadh, Saudi Arabia (1999-2017). We compared patients who had DNR orders during the ICU stay with those with \\\"full code.\\\" The primary outcome was hospital mortality. The secondary outcomes included ICU mortality, tracheostomy, duration of mechanical ventilation, and length of stay in the ICU and hospital.</p><p><strong>Results: </strong>Among 24790 patients admitted to the ICU over the 19-year study period, 3217 (13%) had DNR orders during the ICU stay. Compared to patients with \\\"full code,\\\" patients with DNR orders were older (median 67 years [Q1, Q3: 55, 76] versus 57 years [Q1, Q3: 33, 71], <i>p</i> < 0.0001), were more likely to be females (43% versus 38%, <i>p</i> < 0.0001), had worse premorbid functional status (WHO performance status scores 4-5: 606[18.9%] versus 1894[8.8%], <i>p</i> < 0.0001), higher prevalence of comorbid conditions, and higher APACHE II score (median 28 [Q1, Q3: 23, 34] versus 19 [Q1, Q3: 13, 25], <i>p</i> < 0.0001) and were more likely to be mechanically ventilated (83% versus 55%, <i>p</i> < 0.0001). Patients had DNR orders were more likely to die in the ICU (67.8% versus 8.5%, <i>p</i> < 0.0001) and hospital (82.4% versus 18.1%, <i>p</i> < 0.0001). On multivariable logistic regression analysis, the following were associated with an increased likelihood of DNR status: increasing age (odds ratio (OR) 1.01, 95% confidence interval (CI) 1.01-1.02), higher APACHE II score (OR 1.09, 95% CI 1.08-1.10), and worse WHO performance status score. Patients admitted in recent years (2012-2017 versus 2002-2005) were less likely to have DNR orders (OR 0.35, 95% CI 0.32-0.39, <i>p</i> < 0.0001). Patients with DNR orders had higher ICU mortality, more tracheostomies, longer duration of mechanical ventilation and length of ICU stay compared to patients with with \\\"full code\\\" but they had shorter length of hospital stay.</p><p><strong>Conclusion: </strong>In a tertiary-care hospital in Saudi Arabia, 13% of critically ill patients had DNR orders during ICU stay. This study identified several predictors of DNR orders, including the severity of illness and poor premorbid functional status.</p>\",\"PeriodicalId\":46583,\"journal\":{\"name\":\"Critical Care Research and Practice\",\"volume\":\"2024 \",\"pages\":\"5516516\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-05-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11090671/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/5516516\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/5516516","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Practice and Predictors of Do-Not-Resuscitate Orders in a Tertiary-Care Intensive Care Unit in Saudi Arabia.
Introduction: The objective of this study was to describe Do-Not-Resuscitate (DNR) practices in a tertiary-care intensive care unit (ICU) in Saudi Arabia, and determine the predictors and outcomes of patients who had DNR orders.
Methods: This retrospective cohort study was based on a prospectively collected database for a medical-surgicalIntensive CareDepartment in a tertiary-care center in Riyadh, Saudi Arabia (1999-2017). We compared patients who had DNR orders during the ICU stay with those with "full code." The primary outcome was hospital mortality. The secondary outcomes included ICU mortality, tracheostomy, duration of mechanical ventilation, and length of stay in the ICU and hospital.
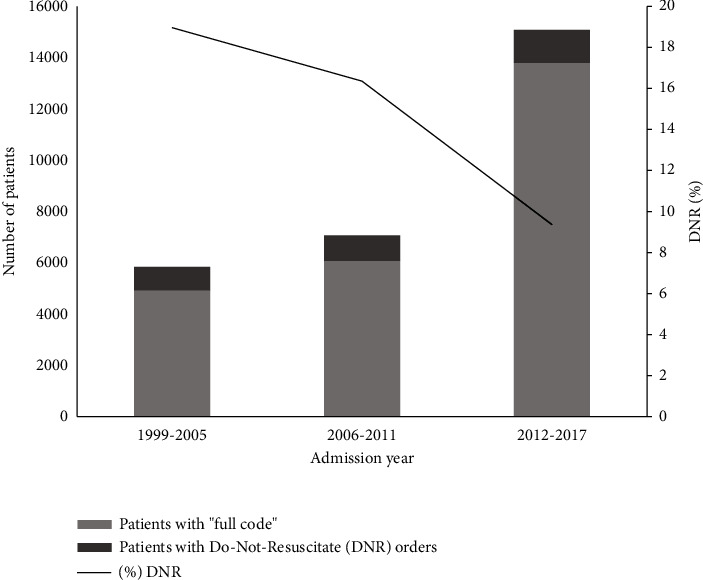
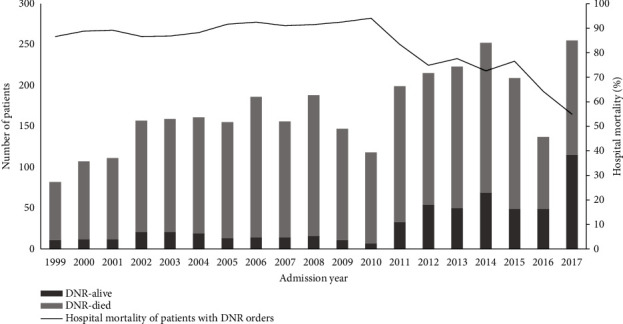
Results: Among 24790 patients admitted to the ICU over the 19-year study period, 3217 (13%) had DNR orders during the ICU stay. Compared to patients with "full code," patients with DNR orders were older (median 67 years [Q1, Q3: 55, 76] versus 57 years [Q1, Q3: 33, 71], p < 0.0001), were more likely to be females (43% versus 38%, p < 0.0001), had worse premorbid functional status (WHO performance status scores 4-5: 606[18.9%] versus 1894[8.8%], p < 0.0001), higher prevalence of comorbid conditions, and higher APACHE II score (median 28 [Q1, Q3: 23, 34] versus 19 [Q1, Q3: 13, 25], p < 0.0001) and were more likely to be mechanically ventilated (83% versus 55%, p < 0.0001). Patients had DNR orders were more likely to die in the ICU (67.8% versus 8.5%, p < 0.0001) and hospital (82.4% versus 18.1%, p < 0.0001). On multivariable logistic regression analysis, the following were associated with an increased likelihood of DNR status: increasing age (odds ratio (OR) 1.01, 95% confidence interval (CI) 1.01-1.02), higher APACHE II score (OR 1.09, 95% CI 1.08-1.10), and worse WHO performance status score. Patients admitted in recent years (2012-2017 versus 2002-2005) were less likely to have DNR orders (OR 0.35, 95% CI 0.32-0.39, p < 0.0001). Patients with DNR orders had higher ICU mortality, more tracheostomies, longer duration of mechanical ventilation and length of ICU stay compared to patients with with "full code" but they had shorter length of hospital stay.
Conclusion: In a tertiary-care hospital in Saudi Arabia, 13% of critically ill patients had DNR orders during ICU stay. This study identified several predictors of DNR orders, including the severity of illness and poor premorbid functional status.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
