{"title":"内窥镜二氧化碳充气治疗恶性结肠肠套叠。","authors":"Kentaro Mochida, Fumiaki Ishibashi, Sho Suzuki","doi":"10.1111/den.14821","DOIUrl":null,"url":null,"abstract":"<p>Intussusception accounts for 1–5% of the causes of intestinal obstruction in adults.<span><sup>1</sup></span> Surgical resection is a radical treatment for malignant colonic intussusception.<span><sup>2</sup></span> However, emergent endoscopy for assessing colonic obstruction is sometimes needed preoperatively.<span><sup>3</sup></span> Endoscopy can be used to temporally resolve intussusception preoperatively, although a detailed procedure has not been reported. This video reports the use of carbon dioxide (CO<sub>2</sub>) insufflation via colonoscopy to repair intussusception due to colorectal cancer.</p><p>A 58-year-old man presented with severe abdominal pain and constipation. Computed tomography (CT) revealed a large mass and a three-layer structure of the sigmoid colon wall with the mesentery wrapped over the rectum, suggesting intussusception of the sigmoid colon (Fig. 1a). No signs of intestinal ischemia or perforation were observed. Colonoscopy was performed without bowel preparations, revealing a large mass overlapping the normal mucosa in the rectum (Fig. 1b). The colonoscope could not access the oral side of the lesion. Insufflation was achieved using CO<sub>2</sub> through the colonoscope. The mass was moved toward the oral side, and the overlapping sigmoid colon wall was gradually released. Type I advanced cancer of the sigmoid colon was observed after intussusception repair (Fig. 2a). Postcolonoscopy CT revealed that the mass moved to the sigmoid colon and the three-layer structure of the colonic wall disappeared (Fig. 2b). Three weeks after colonoscopy, a laparoscopic-assisted sigmoid colon resection was performed, and the final pathological diagnosis was well-differentiated adenocarcinoma of the sigmoid colon (T3, N0, M0, stage IIa) according to the Japanese Classification.<span><sup>4</sup></span></p><p>Although colonic intussusception repair by air insufflation has been reported previously,<span><sup>5</sup></span> this is the first report of a video of colonic intussusception repair using CO<sub>2</sub> insufflation using a colonoscope. This procedure is simple, inexpensive, and effective for avoiding emergency surgery. Therefore, CO<sub>2</sub> insufflation using colonoscopy may be an alternative option for repairing malignant colonic intussusceptions.</p><p>Author S.S. is an Associate Editor of <i>Digestive Endoscopy</i>. Author S.S. received a speaker honorarium from FUJIFILM Corporation. The other authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 7","pages":"859-860"},"PeriodicalIF":4.7000,"publicationDate":"2024-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14821","citationCount":"0","resultStr":"{\"title\":\"Endoscopic carbon dioxide insufflation treating malignant colonic intussusception\",\"authors\":\"Kentaro Mochida, Fumiaki Ishibashi, Sho Suzuki\",\"doi\":\"10.1111/den.14821\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Intussusception accounts for 1–5% of the causes of intestinal obstruction in adults.<span><sup>1</sup></span> Surgical resection is a radical treatment for malignant colonic intussusception.<span><sup>2</sup></span> However, emergent endoscopy for assessing colonic obstruction is sometimes needed preoperatively.<span><sup>3</sup></span> Endoscopy can be used to temporally resolve intussusception preoperatively, although a detailed procedure has not been reported. This video reports the use of carbon dioxide (CO<sub>2</sub>) insufflation via colonoscopy to repair intussusception due to colorectal cancer.</p><p>A 58-year-old man presented with severe abdominal pain and constipation. Computed tomography (CT) revealed a large mass and a three-layer structure of the sigmoid colon wall with the mesentery wrapped over the rectum, suggesting intussusception of the sigmoid colon (Fig. 1a). No signs of intestinal ischemia or perforation were observed. Colonoscopy was performed without bowel preparations, revealing a large mass overlapping the normal mucosa in the rectum (Fig. 1b). The colonoscope could not access the oral side of the lesion. Insufflation was achieved using CO<sub>2</sub> through the colonoscope. The mass was moved toward the oral side, and the overlapping sigmoid colon wall was gradually released. Type I advanced cancer of the sigmoid colon was observed after intussusception repair (Fig. 2a). Postcolonoscopy CT revealed that the mass moved to the sigmoid colon and the three-layer structure of the colonic wall disappeared (Fig. 2b). Three weeks after colonoscopy, a laparoscopic-assisted sigmoid colon resection was performed, and the final pathological diagnosis was well-differentiated adenocarcinoma of the sigmoid colon (T3, N0, M0, stage IIa) according to the Japanese Classification.<span><sup>4</sup></span></p><p>Although colonic intussusception repair by air insufflation has been reported previously,<span><sup>5</sup></span> this is the first report of a video of colonic intussusception repair using CO<sub>2</sub> insufflation using a colonoscope. This procedure is simple, inexpensive, and effective for avoiding emergency surgery. Therefore, CO<sub>2</sub> insufflation using colonoscopy may be an alternative option for repairing malignant colonic intussusceptions.</p><p>Author S.S. is an Associate Editor of <i>Digestive Endoscopy</i>. Author S.S. received a speaker honorarium from FUJIFILM Corporation. The other authors declare no conflict of interest for this article.</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":\"36 7\",\"pages\":\"859-860\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2024-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14821\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14821\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14821","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Intussusception accounts for 1–5% of the causes of intestinal obstruction in adults.1 Surgical resection is a radical treatment for malignant colonic intussusception.2 However, emergent endoscopy for assessing colonic obstruction is sometimes needed preoperatively.3 Endoscopy can be used to temporally resolve intussusception preoperatively, although a detailed procedure has not been reported. This video reports the use of carbon dioxide (CO2) insufflation via colonoscopy to repair intussusception due to colorectal cancer.
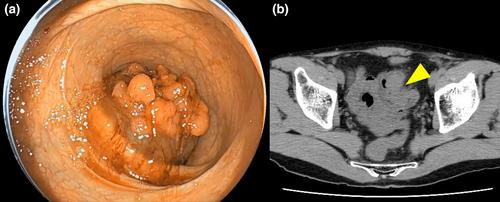
A 58-year-old man presented with severe abdominal pain and constipation. Computed tomography (CT) revealed a large mass and a three-layer structure of the sigmoid colon wall with the mesentery wrapped over the rectum, suggesting intussusception of the sigmoid colon (Fig. 1a). No signs of intestinal ischemia or perforation were observed. Colonoscopy was performed without bowel preparations, revealing a large mass overlapping the normal mucosa in the rectum (Fig. 1b). The colonoscope could not access the oral side of the lesion. Insufflation was achieved using CO2 through the colonoscope. The mass was moved toward the oral side, and the overlapping sigmoid colon wall was gradually released. Type I advanced cancer of the sigmoid colon was observed after intussusception repair (Fig. 2a). Postcolonoscopy CT revealed that the mass moved to the sigmoid colon and the three-layer structure of the colonic wall disappeared (Fig. 2b). Three weeks after colonoscopy, a laparoscopic-assisted sigmoid colon resection was performed, and the final pathological diagnosis was well-differentiated adenocarcinoma of the sigmoid colon (T3, N0, M0, stage IIa) according to the Japanese Classification.4
Although colonic intussusception repair by air insufflation has been reported previously,5 this is the first report of a video of colonic intussusception repair using CO2 insufflation using a colonoscope. This procedure is simple, inexpensive, and effective for avoiding emergency surgery. Therefore, CO2 insufflation using colonoscopy may be an alternative option for repairing malignant colonic intussusceptions.
Author S.S. is an Associate Editor of Digestive Endoscopy. Author S.S. received a speaker honorarium from FUJIFILM Corporation. The other authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
