Jonathan I. Silverberg, Feifei Yang, Evo Alemao, Jing Zhao, Concetta Crivera, Hetal V. Patel, Iris Lin, Aaron R. Mangold
{"title":"美国接受口服皮质类固醇治疗的大疱性类天疱疮患者发生不良事件的风险","authors":"Jonathan I. Silverberg, Feifei Yang, Evo Alemao, Jing Zhao, Concetta Crivera, Hetal V. Patel, Iris Lin, Aaron R. Mangold","doi":"10.1002/jvc2.444","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The potential association of long-term oral corticosteroid (OCS) use with adverse events (AEs) in patients with bullous pemphigoid (BP) is not well characterized in a real-world setting.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>To evaluate the effect of OCS use and treatment duration on the incident AEs in patients with BP.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This retrospective cohort study used medical and pharmacy claims and patient enrollment data from IQVIA PharMetrics® Plus from 2006−2021. Eligible patients had a diagnosis of BP between 1 January 2006 and 30 June 2020 (≥2 claims for BP ≥ 30 days apart). Patients in the OCS cohort also had a claim for OCS use, ≥7.5 mg daily dose of prednisone or equivalent, and no claims for a nonoral systemic corticosteroid (CS) at any time during the study period. A control cohort of patients with BP not using OCS was also selected. Relative risk ratios were estimated between the incidence of AEs in OCS users with different exposure durations (short-term, <30 days; medium-term, 30−90 days; long-term, >90 days) and nonusers by Poisson regression, after adjusting for age, sex, prior drug use, and baseline Charlson Comorbidity Index score within the follow-up period.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>At the 1-year follow-up, long-term OCS users had a higher incidence of infections, cataract, osteoporosis, heart failure, depression or anxiety, and diabetes compared with OCS nonusers (<i>p</i> < 0.05). Furthermore, compared with nonusers, long-term users had increased 1-year risks (risk ratio; 95% confidence interval) for heart failure (2.27; 1.50−3.44), diabetes (2.05; 1.30−3.24), osteoporosis (1.72; 1.23−2.41), and infection (1.50; 1.13−1.99). Long-term OCS users also had increased 1-year risks for heart failure (2.00; 1.21−3.28) and osteoporosis (1.70; 1.16−2.50) compared with short-term OCS users.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Long-term OCS use (≥7.5 mg) in patients with BP was associated with an increased risk of AEs. Study findings demonstrate a need for steroid-sparing options with an improved safety profile.</p>\n </section>\n </div>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 4","pages":"1206-1211"},"PeriodicalIF":0.5000,"publicationDate":"2024-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.444","citationCount":"0","resultStr":"{\"title\":\"Risk of adverse events in patients with bullous pemphigoid treated with oral corticosteroids in the United States\",\"authors\":\"Jonathan I. Silverberg, Feifei Yang, Evo Alemao, Jing Zhao, Concetta Crivera, Hetal V. Patel, Iris Lin, Aaron R. Mangold\",\"doi\":\"10.1002/jvc2.444\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>The potential association of long-term oral corticosteroid (OCS) use with adverse events (AEs) in patients with bullous pemphigoid (BP) is not well characterized in a real-world setting.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>To evaluate the effect of OCS use and treatment duration on the incident AEs in patients with BP.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This retrospective cohort study used medical and pharmacy claims and patient enrollment data from IQVIA PharMetrics® Plus from 2006−2021. Eligible patients had a diagnosis of BP between 1 January 2006 and 30 June 2020 (≥2 claims for BP ≥ 30 days apart). Patients in the OCS cohort also had a claim for OCS use, ≥7.5 mg daily dose of prednisone or equivalent, and no claims for a nonoral systemic corticosteroid (CS) at any time during the study period. A control cohort of patients with BP not using OCS was also selected. Relative risk ratios were estimated between the incidence of AEs in OCS users with different exposure durations (short-term, <30 days; medium-term, 30−90 days; long-term, >90 days) and nonusers by Poisson regression, after adjusting for age, sex, prior drug use, and baseline Charlson Comorbidity Index score within the follow-up period.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>At the 1-year follow-up, long-term OCS users had a higher incidence of infections, cataract, osteoporosis, heart failure, depression or anxiety, and diabetes compared with OCS nonusers (<i>p</i> < 0.05). Furthermore, compared with nonusers, long-term users had increased 1-year risks (risk ratio; 95% confidence interval) for heart failure (2.27; 1.50−3.44), diabetes (2.05; 1.30−3.24), osteoporosis (1.72; 1.23−2.41), and infection (1.50; 1.13−1.99). Long-term OCS users also had increased 1-year risks for heart failure (2.00; 1.21−3.28) and osteoporosis (1.70; 1.16−2.50) compared with short-term OCS users.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Long-term OCS use (≥7.5 mg) in patients with BP was associated with an increased risk of AEs. Study findings demonstrate a need for steroid-sparing options with an improved safety profile.</p>\\n </section>\\n </div>\",\"PeriodicalId\":94325,\"journal\":{\"name\":\"JEADV clinical practice\",\"volume\":\"3 4\",\"pages\":\"1206-1211\"},\"PeriodicalIF\":0.5000,\"publicationDate\":\"2024-05-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.444\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JEADV clinical practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.444\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.444","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Risk of adverse events in patients with bullous pemphigoid treated with oral corticosteroids in the United States
Background
The potential association of long-term oral corticosteroid (OCS) use with adverse events (AEs) in patients with bullous pemphigoid (BP) is not well characterized in a real-world setting.
Objectives
To evaluate the effect of OCS use and treatment duration on the incident AEs in patients with BP.
Methods
This retrospective cohort study used medical and pharmacy claims and patient enrollment data from IQVIA PharMetrics® Plus from 2006−2021. Eligible patients had a diagnosis of BP between 1 January 2006 and 30 June 2020 (≥2 claims for BP ≥ 30 days apart). Patients in the OCS cohort also had a claim for OCS use, ≥7.5 mg daily dose of prednisone or equivalent, and no claims for a nonoral systemic corticosteroid (CS) at any time during the study period. A control cohort of patients with BP not using OCS was also selected. Relative risk ratios were estimated between the incidence of AEs in OCS users with different exposure durations (short-term, <30 days; medium-term, 30−90 days; long-term, >90 days) and nonusers by Poisson regression, after adjusting for age, sex, prior drug use, and baseline Charlson Comorbidity Index score within the follow-up period.
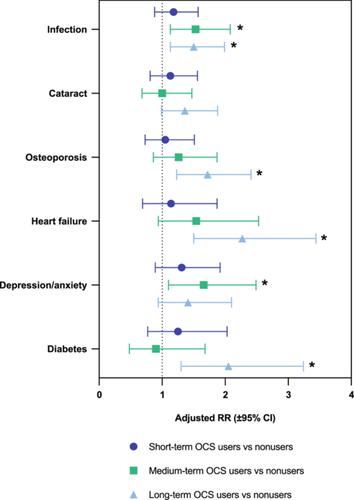
Results
At the 1-year follow-up, long-term OCS users had a higher incidence of infections, cataract, osteoporosis, heart failure, depression or anxiety, and diabetes compared with OCS nonusers (p < 0.05). Furthermore, compared with nonusers, long-term users had increased 1-year risks (risk ratio; 95% confidence interval) for heart failure (2.27; 1.50−3.44), diabetes (2.05; 1.30−3.24), osteoporosis (1.72; 1.23−2.41), and infection (1.50; 1.13−1.99). Long-term OCS users also had increased 1-year risks for heart failure (2.00; 1.21−3.28) and osteoporosis (1.70; 1.16−2.50) compared with short-term OCS users.
Conclusions
Long-term OCS use (≥7.5 mg) in patients with BP was associated with an increased risk of AEs. Study findings demonstrate a need for steroid-sparing options with an improved safety profile.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
