{"title":"嗜酸性粒细胞食管炎的药物治疗。","authors":"Hannah F. Marshall, Melvin Lee Qiyu","doi":"10.1111/cea.14509","DOIUrl":null,"url":null,"abstract":"<p>Eosinophilic esophagitis (EoE) is a chronic inflammatory condition of the oesophagus first described in the 1970s.<span><sup>1</sup></span> All ages can be affected; however, it is more common in males and adults. Estimates of incidence in Europe and the United States range from 1.3 to 12.8 cases per 100,000.<span><sup>2</sup></span></p><p>Presenting symptoms vary widely between patients, including dysphagia, pain and food bolus impaction/obstruction.<span><sup>1-3</sup></span> EoE often coexists with other atopic diseases, and evidence supports an underlying mechanism of type-2 inflammatory response to food antigens.<span><sup>1, 2</sup></span> Diagnosis is made with a peak eosinophil count of ≥15 eosinophils/0.3 mm<sup>2</sup> on oesophageal histology.<span><sup>1, 3</sup></span> Recently, a group in France published on their automated, accurate and reproducible method to assess eosinophilic density and degree of degranulation, which poses time-saving advantages.<span><sup>4</sup></span></p><p>Treatment of EoE is lifelong, aiming to prevent fibrostenosis and strictures.<span><sup>3</sup></span> Elimination diets and corticosteroids have been used for many years, and biologics are now available for some patients. This Cochrane Corner will summarize the effectiveness and safety of medical interventions for people with EoE and put these in a useful, clinical context for the practising clinician.</p><p>This review comprised 41 RCTs involving 3253 participants with EoE. The primary interventions evaluated were corticosteroids versus placebo and biologics versus placebo; however, the review incorporated RCTs examining 19 intervention–comparisons of dietary modification or medication, including leukotriene receptor antagonists and transcutaneous patches. While children and adults were included, the authors felt the evidence had limited applicability to under 18 s.<span><sup>1</sup></span></p><p>For induction of remission, the authors concluded that corticosteroids improve histologic outcomes, and biologic anti-IL13 and anti-IL4r therapies may improve clinical outcomes (Figure 1). With no head-to-head trials, factors such as cost, acceptability and the burden of treatment are important to consider.</p><p>Budesonide respules (1 mg twice-daily) are estimated $2316/quarter, with fluticasone (440 mcg twice-daily) costing $691/quarter.<span><sup>5</sup></span> Comparatively, a quarterly supply of dupilumab (300 mg weekly), the only biologic currently licensed for EoE (US and EU, not UK, for over 12 s weighing >40 kg) would cost around $15,600.<span><sup>6</sup></span></p><p>A six-food elimination diet is estimated to cost around $710/quarter for a single male living alone, and patients need to visit multiple stores to purchase a nutritionally balanced grocery shop.<span><sup>7</sup></span> Hidden expenses affect patients on elimination diets as they require more endoscopies than those on corticosteroids, costing more in missed working hours and hospital visits, depending on the healthcare system.<span><sup>1, 5</sup></span></p><p>This economic discrepancy would likely play a crucial role in treatment planning, potentially limiting options for patients in insurance/self-pay healthcare systems. Despite many biologics appearing on the WHO essential medicines list, they are amongst the most expensive medicines in the world and remain difficult to access.<span><sup>8</sup></span></p><p>Both primary interventions were found to be acceptable to patients, and patients on both were just as likely to experience adverse events as those on placebo.<span><sup>1</sup></span> The most common side effect of topical corticosteroids is oral/oesophageal candidiasis<span><sup>3</sup></span> and of dupilumab is injection site reactions or ocular surface disease (OSD). The latter is seen less with anti-IL13 tralokinumab.<span><sup>6, 9</sup></span></p><p>Further head-to-head trials and cost-effectiveness analyses are necessary to fully evaluate and compare corticosteroids and biologics in the treatment of EoE.</p><p>Both authors contributed equally to this manuscript.</p><p>No funders available.</p><p>The authors have no conflicts of interest to declare.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 6","pages":"374-377"},"PeriodicalIF":5.0000,"publicationDate":"2024-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14509","citationCount":"0","resultStr":"{\"title\":\"Medical treatment of eosinophilic esophagitis\",\"authors\":\"Hannah F. Marshall, Melvin Lee Qiyu\",\"doi\":\"10.1111/cea.14509\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Eosinophilic esophagitis (EoE) is a chronic inflammatory condition of the oesophagus first described in the 1970s.<span><sup>1</sup></span> All ages can be affected; however, it is more common in males and adults. Estimates of incidence in Europe and the United States range from 1.3 to 12.8 cases per 100,000.<span><sup>2</sup></span></p><p>Presenting symptoms vary widely between patients, including dysphagia, pain and food bolus impaction/obstruction.<span><sup>1-3</sup></span> EoE often coexists with other atopic diseases, and evidence supports an underlying mechanism of type-2 inflammatory response to food antigens.<span><sup>1, 2</sup></span> Diagnosis is made with a peak eosinophil count of ≥15 eosinophils/0.3 mm<sup>2</sup> on oesophageal histology.<span><sup>1, 3</sup></span> Recently, a group in France published on their automated, accurate and reproducible method to assess eosinophilic density and degree of degranulation, which poses time-saving advantages.<span><sup>4</sup></span></p><p>Treatment of EoE is lifelong, aiming to prevent fibrostenosis and strictures.<span><sup>3</sup></span> Elimination diets and corticosteroids have been used for many years, and biologics are now available for some patients. This Cochrane Corner will summarize the effectiveness and safety of medical interventions for people with EoE and put these in a useful, clinical context for the practising clinician.</p><p>This review comprised 41 RCTs involving 3253 participants with EoE. The primary interventions evaluated were corticosteroids versus placebo and biologics versus placebo; however, the review incorporated RCTs examining 19 intervention–comparisons of dietary modification or medication, including leukotriene receptor antagonists and transcutaneous patches. While children and adults were included, the authors felt the evidence had limited applicability to under 18 s.<span><sup>1</sup></span></p><p>For induction of remission, the authors concluded that corticosteroids improve histologic outcomes, and biologic anti-IL13 and anti-IL4r therapies may improve clinical outcomes (Figure 1). With no head-to-head trials, factors such as cost, acceptability and the burden of treatment are important to consider.</p><p>Budesonide respules (1 mg twice-daily) are estimated $2316/quarter, with fluticasone (440 mcg twice-daily) costing $691/quarter.<span><sup>5</sup></span> Comparatively, a quarterly supply of dupilumab (300 mg weekly), the only biologic currently licensed for EoE (US and EU, not UK, for over 12 s weighing >40 kg) would cost around $15,600.<span><sup>6</sup></span></p><p>A six-food elimination diet is estimated to cost around $710/quarter for a single male living alone, and patients need to visit multiple stores to purchase a nutritionally balanced grocery shop.<span><sup>7</sup></span> Hidden expenses affect patients on elimination diets as they require more endoscopies than those on corticosteroids, costing more in missed working hours and hospital visits, depending on the healthcare system.<span><sup>1, 5</sup></span></p><p>This economic discrepancy would likely play a crucial role in treatment planning, potentially limiting options for patients in insurance/self-pay healthcare systems. Despite many biologics appearing on the WHO essential medicines list, they are amongst the most expensive medicines in the world and remain difficult to access.<span><sup>8</sup></span></p><p>Both primary interventions were found to be acceptable to patients, and patients on both were just as likely to experience adverse events as those on placebo.<span><sup>1</sup></span> The most common side effect of topical corticosteroids is oral/oesophageal candidiasis<span><sup>3</sup></span> and of dupilumab is injection site reactions or ocular surface disease (OSD). The latter is seen less with anti-IL13 tralokinumab.<span><sup>6, 9</sup></span></p><p>Further head-to-head trials and cost-effectiveness analyses are necessary to fully evaluate and compare corticosteroids and biologics in the treatment of EoE.</p><p>Both authors contributed equally to this manuscript.</p><p>No funders available.</p><p>The authors have no conflicts of interest to declare.</p>\",\"PeriodicalId\":10207,\"journal\":{\"name\":\"Clinical and Experimental Allergy\",\"volume\":\"54 6\",\"pages\":\"374-377\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-05-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14509\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cea.14509\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14509","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
Eosinophilic esophagitis (EoE) is a chronic inflammatory condition of the oesophagus first described in the 1970s.1 All ages can be affected; however, it is more common in males and adults. Estimates of incidence in Europe and the United States range from 1.3 to 12.8 cases per 100,000.2
Presenting symptoms vary widely between patients, including dysphagia, pain and food bolus impaction/obstruction.1-3 EoE often coexists with other atopic diseases, and evidence supports an underlying mechanism of type-2 inflammatory response to food antigens.1, 2 Diagnosis is made with a peak eosinophil count of ≥15 eosinophils/0.3 mm2 on oesophageal histology.1, 3 Recently, a group in France published on their automated, accurate and reproducible method to assess eosinophilic density and degree of degranulation, which poses time-saving advantages.4
Treatment of EoE is lifelong, aiming to prevent fibrostenosis and strictures.3 Elimination diets and corticosteroids have been used for many years, and biologics are now available for some patients. This Cochrane Corner will summarize the effectiveness and safety of medical interventions for people with EoE and put these in a useful, clinical context for the practising clinician.
This review comprised 41 RCTs involving 3253 participants with EoE. The primary interventions evaluated were corticosteroids versus placebo and biologics versus placebo; however, the review incorporated RCTs examining 19 intervention–comparisons of dietary modification or medication, including leukotriene receptor antagonists and transcutaneous patches. While children and adults were included, the authors felt the evidence had limited applicability to under 18 s.1
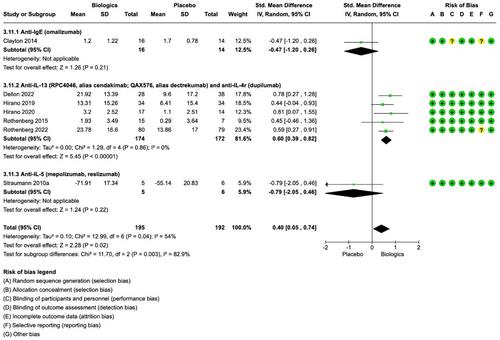
For induction of remission, the authors concluded that corticosteroids improve histologic outcomes, and biologic anti-IL13 and anti-IL4r therapies may improve clinical outcomes (Figure 1). With no head-to-head trials, factors such as cost, acceptability and the burden of treatment are important to consider.
Budesonide respules (1 mg twice-daily) are estimated $2316/quarter, with fluticasone (440 mcg twice-daily) costing $691/quarter.5 Comparatively, a quarterly supply of dupilumab (300 mg weekly), the only biologic currently licensed for EoE (US and EU, not UK, for over 12 s weighing >40 kg) would cost around $15,600.6
A six-food elimination diet is estimated to cost around $710/quarter for a single male living alone, and patients need to visit multiple stores to purchase a nutritionally balanced grocery shop.7 Hidden expenses affect patients on elimination diets as they require more endoscopies than those on corticosteroids, costing more in missed working hours and hospital visits, depending on the healthcare system.1, 5
This economic discrepancy would likely play a crucial role in treatment planning, potentially limiting options for patients in insurance/self-pay healthcare systems. Despite many biologics appearing on the WHO essential medicines list, they are amongst the most expensive medicines in the world and remain difficult to access.8
Both primary interventions were found to be acceptable to patients, and patients on both were just as likely to experience adverse events as those on placebo.1 The most common side effect of topical corticosteroids is oral/oesophageal candidiasis3 and of dupilumab is injection site reactions or ocular surface disease (OSD). The latter is seen less with anti-IL13 tralokinumab.6, 9
Further head-to-head trials and cost-effectiveness analyses are necessary to fully evaluate and compare corticosteroids and biologics in the treatment of EoE.
Both authors contributed equally to this manuscript.
No funders available.
The authors have no conflicts of interest to declare.
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
