Jennifer M. Ross, Chelsea Greene, Cara J. Broshkevitch, David W. Dowdy, Alastair van Heerden, Jesse Heitner, Darcy W. Rao, D. Allen Roberts, Adrienne E. Shapiro, Zelda B. Zabinsky, Ruanne V. Barnabas
{"title":"在艾滋病毒流行的环境中通过社区护理预防结核病:模型分析。","authors":"Jennifer M. Ross, Chelsea Greene, Cara J. Broshkevitch, David W. Dowdy, Alastair van Heerden, Jesse Heitner, Darcy W. Rao, D. Allen Roberts, Adrienne E. Shapiro, Zelda B. Zabinsky, Ruanne V. Barnabas","doi":"10.1002/jia2.26272","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Antiretroviral therapy (ART) and tuberculosis preventive treatment (TPT) both prevent tuberculosis (TB) disease and deaths among people living with HIV. Differentiated care models, including community-based care, can increase the uptake of ART and TPT to prevent TB in settings with a high burden of HIV-associated TB, particularly among men.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We developed a gender-stratified dynamic model of TB and HIV transmission and disease progression among 100,000 adults ages 15−59 in KwaZulu-Natal, South Africa. We drew model parameters from a community-based ART initiation and resupply trial in sub-Saharan Africa (Delivery Optimization for Antiretroviral Therapy, DO ART) and other scientific literature. We simulated the impacts of community-based ART and TPT care programmes during 2018−2027, assuming that community-based ART and TPT care were scaled up to similar levels as in the DO ART trial (i.e. ART coverage increasing from 49% to 82% among men and from 69% to 83% among women) and sustained for 10 years. We projected the number of TB cases, deaths and disability-adjusted life years (DALYs) averted relative to standard, clinic-based care. We calculated programme costs and incremental cost-effectiveness ratios from the provider perspective.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>If community-based ART care could be implemented with similar effectiveness to the DO ART trial, increased ART coverage could reduce TB incidence by 27.0% (range 21.3%−34.1%) and TB mortality by 34.6% (range 24.8%–42.2%) after 10 years. Increasing both ART and TPT uptake through community-based ART with TPT care could reduce TB incidence by 29.7% (range 23.9%−36.0%) and TB mortality by 36.0% (range 26.9%−43.8%). Community-based ART with TPT care reduced gender disparities in TB mortality rates, with a projected 54 more deaths annually among men than women (range 11–103) after 10 years of community-based care versus 109 (range 41–182) in standard care. Over 10 years, the mean cost per DALY averted by community-based ART with TPT care was $846 USD (range $709–$1012).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>By substantially increasing coverage of ART and TPT, community-based care for people living with HIV could reduce TB incidence and mortality in settings with high burdens of HIV-associated TB and reduce TB gender disparities.</p>\n </section>\n </div>","PeriodicalId":201,"journal":{"name":"Journal of the International AIDS Society","volume":"27 6","pages":""},"PeriodicalIF":4.9000,"publicationDate":"2024-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jia2.26272","citationCount":"0","resultStr":"{\"title\":\"Preventing tuberculosis with community-based care in an HIV-endemic setting: a modelling analysis\",\"authors\":\"Jennifer M. Ross, Chelsea Greene, Cara J. Broshkevitch, David W. Dowdy, Alastair van Heerden, Jesse Heitner, Darcy W. Rao, D. Allen Roberts, Adrienne E. Shapiro, Zelda B. Zabinsky, Ruanne V. Barnabas\",\"doi\":\"10.1002/jia2.26272\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>Antiretroviral therapy (ART) and tuberculosis preventive treatment (TPT) both prevent tuberculosis (TB) disease and deaths among people living with HIV. Differentiated care models, including community-based care, can increase the uptake of ART and TPT to prevent TB in settings with a high burden of HIV-associated TB, particularly among men.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We developed a gender-stratified dynamic model of TB and HIV transmission and disease progression among 100,000 adults ages 15−59 in KwaZulu-Natal, South Africa. We drew model parameters from a community-based ART initiation and resupply trial in sub-Saharan Africa (Delivery Optimization for Antiretroviral Therapy, DO ART) and other scientific literature. We simulated the impacts of community-based ART and TPT care programmes during 2018−2027, assuming that community-based ART and TPT care were scaled up to similar levels as in the DO ART trial (i.e. ART coverage increasing from 49% to 82% among men and from 69% to 83% among women) and sustained for 10 years. We projected the number of TB cases, deaths and disability-adjusted life years (DALYs) averted relative to standard, clinic-based care. We calculated programme costs and incremental cost-effectiveness ratios from the provider perspective.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>If community-based ART care could be implemented with similar effectiveness to the DO ART trial, increased ART coverage could reduce TB incidence by 27.0% (range 21.3%−34.1%) and TB mortality by 34.6% (range 24.8%–42.2%) after 10 years. Increasing both ART and TPT uptake through community-based ART with TPT care could reduce TB incidence by 29.7% (range 23.9%−36.0%) and TB mortality by 36.0% (range 26.9%−43.8%). Community-based ART with TPT care reduced gender disparities in TB mortality rates, with a projected 54 more deaths annually among men than women (range 11–103) after 10 years of community-based care versus 109 (range 41–182) in standard care. Over 10 years, the mean cost per DALY averted by community-based ART with TPT care was $846 USD (range $709–$1012).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>By substantially increasing coverage of ART and TPT, community-based care for people living with HIV could reduce TB incidence and mortality in settings with high burdens of HIV-associated TB and reduce TB gender disparities.</p>\\n </section>\\n </div>\",\"PeriodicalId\":201,\"journal\":{\"name\":\"Journal of the International AIDS Society\",\"volume\":\"27 6\",\"pages\":\"\"},\"PeriodicalIF\":4.9000,\"publicationDate\":\"2024-06-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jia2.26272\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the International AIDS Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jia2.26272\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the International AIDS Society","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jia2.26272","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
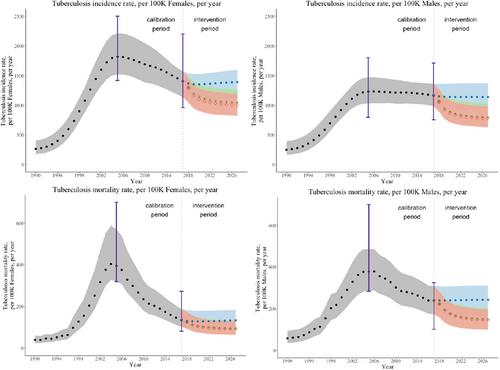
Preventing tuberculosis with community-based care in an HIV-endemic setting: a modelling analysis
Introduction
Antiretroviral therapy (ART) and tuberculosis preventive treatment (TPT) both prevent tuberculosis (TB) disease and deaths among people living with HIV. Differentiated care models, including community-based care, can increase the uptake of ART and TPT to prevent TB in settings with a high burden of HIV-associated TB, particularly among men.
Methods
We developed a gender-stratified dynamic model of TB and HIV transmission and disease progression among 100,000 adults ages 15−59 in KwaZulu-Natal, South Africa. We drew model parameters from a community-based ART initiation and resupply trial in sub-Saharan Africa (Delivery Optimization for Antiretroviral Therapy, DO ART) and other scientific literature. We simulated the impacts of community-based ART and TPT care programmes during 2018−2027, assuming that community-based ART and TPT care were scaled up to similar levels as in the DO ART trial (i.e. ART coverage increasing from 49% to 82% among men and from 69% to 83% among women) and sustained for 10 years. We projected the number of TB cases, deaths and disability-adjusted life years (DALYs) averted relative to standard, clinic-based care. We calculated programme costs and incremental cost-effectiveness ratios from the provider perspective.
Results
If community-based ART care could be implemented with similar effectiveness to the DO ART trial, increased ART coverage could reduce TB incidence by 27.0% (range 21.3%−34.1%) and TB mortality by 34.6% (range 24.8%–42.2%) after 10 years. Increasing both ART and TPT uptake through community-based ART with TPT care could reduce TB incidence by 29.7% (range 23.9%−36.0%) and TB mortality by 36.0% (range 26.9%−43.8%). Community-based ART with TPT care reduced gender disparities in TB mortality rates, with a projected 54 more deaths annually among men than women (range 11–103) after 10 years of community-based care versus 109 (range 41–182) in standard care. Over 10 years, the mean cost per DALY averted by community-based ART with TPT care was $846 USD (range $709–$1012).
Conclusions
By substantially increasing coverage of ART and TPT, community-based care for people living with HIV could reduce TB incidence and mortality in settings with high burdens of HIV-associated TB and reduce TB gender disparities.
期刊介绍:
The Journal of the International AIDS Society (JIAS) is a peer-reviewed and Open Access journal for the generation and dissemination of evidence from a wide range of disciplines: basic and biomedical sciences; behavioural sciences; epidemiology; clinical sciences; health economics and health policy; operations research and implementation sciences; and social sciences and humanities. Submission of HIV research carried out in low- and middle-income countries is strongly encouraged.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
