Malcolm L. McDonald MD, Yosef Manla MD, Alice Sonnino MD, Mileydis Alonso DO, Radhika K. Neicheril MD, Alejandro Sanchez MD, Gabrielle Lafave MD, Yelenis Seijo De Armas MD, Antonio Lewis Camargo MD, Dipan Uppal MD, Armaan Handa MS, David Wolinsky MD, Nina Thakkar Rivera DO, PhD, Mauricio Velez MD, David A. Baran MD, Jerry D. Estep MD, David Snipelisky MD
{"title":"转甲状腺素心脏淀粉样变性确诊后出现肾功能障碍的预测因素。","authors":"Malcolm L. McDonald MD, Yosef Manla MD, Alice Sonnino MD, Mileydis Alonso DO, Radhika K. Neicheril MD, Alejandro Sanchez MD, Gabrielle Lafave MD, Yelenis Seijo De Armas MD, Antonio Lewis Camargo MD, Dipan Uppal MD, Armaan Handa MS, David Wolinsky MD, Nina Thakkar Rivera DO, PhD, Mauricio Velez MD, David A. Baran MD, Jerry D. Estep MD, David Snipelisky MD","doi":"10.1002/clc.24298","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>In patients with transthyretin cardiac amyloidosis (ATTR-CA), renal dysfunction is a poor prognostic indicator. Limited data are available on variables that portend worsening renal function (wRF) among ATTR-CA patients.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>This study assesses which characteristics place patients at higher risk for the development of wRF (defined as a drop of ≥10% in glomerular filtration rate [GFR]) within the first year following diagnosis of ATTR-CA.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We included patients with ATTR-CA (<i>n</i> = 134) evaluated between 2/2016 and 12/2022 and followed for up to 1 year at our amyloid clinic. Patients were stratified into two groups: a group with maintained renal function (mRF) and a group with wRF and compared using appropriate testing. Significant variables in the univariate analysis were included in the multivariable logistic regression model to determine characteristics associated with wRF.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Within a follow-up period of 326 ± 118 days, the median GFR% change measured −6% [−18%, +8]. About 41.8% (<i>n</i> = 56) had wRF, while the remainder had mRF. In addition, in patients with no prior history of chronic kidney disease (CKD), 25.5% developed de novo CKD. On multivariable logistic regression, only New York Heart Association (NYHA) class ≥III (odds ratio [OR]: 3.9, 95% confidence interval [CI]: [1.6–9.3]), history of ischemic heart disease (IHD) (OR: 0.3, 95% CI: [0.1–0.7]), and not receiving SGLT-2i (OR: 0.1, 95% CI: [0.02–0.5]) were significant predictors of wRF.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Our study demonstrated that the development of de novo renal dysfunction or wRF is common following the diagnosis of ATTR-CA. Additionally, we identified worse NYHA class and no prior history of IHD as significant predictors associated with developing wRF, while receiving SGLT-2i therapy appeared to be protective in this population.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 6","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2024-06-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24298","citationCount":"0","resultStr":"{\"title\":\"Predictors of developing renal dysfunction following diagnosis of transthyretin cardiac amyloidosis\",\"authors\":\"Malcolm L. McDonald MD, Yosef Manla MD, Alice Sonnino MD, Mileydis Alonso DO, Radhika K. Neicheril MD, Alejandro Sanchez MD, Gabrielle Lafave MD, Yelenis Seijo De Armas MD, Antonio Lewis Camargo MD, Dipan Uppal MD, Armaan Handa MS, David Wolinsky MD, Nina Thakkar Rivera DO, PhD, Mauricio Velez MD, David A. Baran MD, Jerry D. Estep MD, David Snipelisky MD\",\"doi\":\"10.1002/clc.24298\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>In patients with transthyretin cardiac amyloidosis (ATTR-CA), renal dysfunction is a poor prognostic indicator. Limited data are available on variables that portend worsening renal function (wRF) among ATTR-CA patients.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>This study assesses which characteristics place patients at higher risk for the development of wRF (defined as a drop of ≥10% in glomerular filtration rate [GFR]) within the first year following diagnosis of ATTR-CA.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We included patients with ATTR-CA (<i>n</i> = 134) evaluated between 2/2016 and 12/2022 and followed for up to 1 year at our amyloid clinic. Patients were stratified into two groups: a group with maintained renal function (mRF) and a group with wRF and compared using appropriate testing. Significant variables in the univariate analysis were included in the multivariable logistic regression model to determine characteristics associated with wRF.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Within a follow-up period of 326 ± 118 days, the median GFR% change measured −6% [−18%, +8]. About 41.8% (<i>n</i> = 56) had wRF, while the remainder had mRF. In addition, in patients with no prior history of chronic kidney disease (CKD), 25.5% developed de novo CKD. On multivariable logistic regression, only New York Heart Association (NYHA) class ≥III (odds ratio [OR]: 3.9, 95% confidence interval [CI]: [1.6–9.3]), history of ischemic heart disease (IHD) (OR: 0.3, 95% CI: [0.1–0.7]), and not receiving SGLT-2i (OR: 0.1, 95% CI: [0.02–0.5]) were significant predictors of wRF.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Our study demonstrated that the development of de novo renal dysfunction or wRF is common following the diagnosis of ATTR-CA. Additionally, we identified worse NYHA class and no prior history of IHD as significant predictors associated with developing wRF, while receiving SGLT-2i therapy appeared to be protective in this population.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10201,\"journal\":{\"name\":\"Clinical Cardiology\",\"volume\":\"47 6\",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-06-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24298\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.24298\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.24298","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Predictors of developing renal dysfunction following diagnosis of transthyretin cardiac amyloidosis
Background
In patients with transthyretin cardiac amyloidosis (ATTR-CA), renal dysfunction is a poor prognostic indicator. Limited data are available on variables that portend worsening renal function (wRF) among ATTR-CA patients.
Objectives
This study assesses which characteristics place patients at higher risk for the development of wRF (defined as a drop of ≥10% in glomerular filtration rate [GFR]) within the first year following diagnosis of ATTR-CA.
Methods
We included patients with ATTR-CA (n = 134) evaluated between 2/2016 and 12/2022 and followed for up to 1 year at our amyloid clinic. Patients were stratified into two groups: a group with maintained renal function (mRF) and a group with wRF and compared using appropriate testing. Significant variables in the univariate analysis were included in the multivariable logistic regression model to determine characteristics associated with wRF.
Results
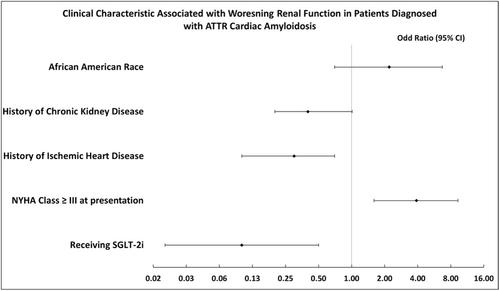
Within a follow-up period of 326 ± 118 days, the median GFR% change measured −6% [−18%, +8]. About 41.8% (n = 56) had wRF, while the remainder had mRF. In addition, in patients with no prior history of chronic kidney disease (CKD), 25.5% developed de novo CKD. On multivariable logistic regression, only New York Heart Association (NYHA) class ≥III (odds ratio [OR]: 3.9, 95% confidence interval [CI]: [1.6–9.3]), history of ischemic heart disease (IHD) (OR: 0.3, 95% CI: [0.1–0.7]), and not receiving SGLT-2i (OR: 0.1, 95% CI: [0.02–0.5]) were significant predictors of wRF.
Conclusion
Our study demonstrated that the development of de novo renal dysfunction or wRF is common following the diagnosis of ATTR-CA. Additionally, we identified worse NYHA class and no prior history of IHD as significant predictors associated with developing wRF, while receiving SGLT-2i therapy appeared to be protective in this population.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
