Rajendra Aldis, Lisa C. Rosenfeld, Norah Mulvaney-Day, Margaret Lanca, Kate Zona, Jeffrey A. Lam, Julia Asfour, Jonah C. Meltzer, H. Stephen Leff, Carl Fulwiler, Philip Wang, Ana M. Progovac
{"title":"作为学习型医疗系统过渡的一部分,安全网门诊精神病科采用基于远程测量的护理的决定因素","authors":"Rajendra Aldis, Lisa C. Rosenfeld, Norah Mulvaney-Day, Margaret Lanca, Kate Zona, Jeffrey A. Lam, Julia Asfour, Jonah C. Meltzer, H. Stephen Leff, Carl Fulwiler, Philip Wang, Ana M. Progovac","doi":"10.1002/lrh2.10416","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Behavioral measurement-based care (MBC) can improve patient outcomes and has also been advanced as a critical learning health system (LHS) tool for identifying and mitigating potential disparities in mental health treatment. However, little is known about the uptake of remote behavioral MBC in safety net settings, or possible disparities occurring in remote MBC implementation.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This study uses electronic health record data to study variation in completion rates at the clinic and patient level of a remote MBC symptom measure tool during the first 6 months of implementation at three adult outpatient psychiatry clinics in a safety net health system. Provider-reported barriers to MBC adoption were also measured using repeated surveys at one of the three sites.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Out of 1219 patients who were sent an MBC measure request, uptake of completing at least one measure varied by clinic: General Adult Clinic, 38% (n = 262 of 696); Substance Use Clinic, 28% (n = 73 of 265); and Transitions Clinic, 17% (n = 44 of 258). Compared with White patients, Black and Portuguese or Brazilian patients had lower uptake. Older patients also had lower uptake. Spanish language of care was associated with much lower uptake at the patient level. Significant patient-level disparities in uptake persisted after adjusting for the clinic, mental health diagnoses, and number of measure requests sent. Providers cited time within visits and bandwidth in their workflow as the greatest consistent barriers to discussing MBC results with patients.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>There are significant disparities in MBC uptake at the patient and clinic level. From an LHS data infrastructure perspective, safety net health systems may need to address the need for possible ways to adapt MBC to better fit their populations and clinical needs, or identify targeted implementation strategies to close data gaps for the identified disparity populations.</p>\n </section>\n </div>","PeriodicalId":43916,"journal":{"name":"Learning Health Systems","volume":"8 S1","pages":""},"PeriodicalIF":2.6000,"publicationDate":"2024-04-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10416","citationCount":"0","resultStr":"{\"title\":\"Determinants of remote measurement-based care uptake in a safety net outpatient psychiatry department as part of learning health system transition\",\"authors\":\"Rajendra Aldis, Lisa C. Rosenfeld, Norah Mulvaney-Day, Margaret Lanca, Kate Zona, Jeffrey A. Lam, Julia Asfour, Jonah C. Meltzer, H. Stephen Leff, Carl Fulwiler, Philip Wang, Ana M. Progovac\",\"doi\":\"10.1002/lrh2.10416\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>Behavioral measurement-based care (MBC) can improve patient outcomes and has also been advanced as a critical learning health system (LHS) tool for identifying and mitigating potential disparities in mental health treatment. However, little is known about the uptake of remote behavioral MBC in safety net settings, or possible disparities occurring in remote MBC implementation.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This study uses electronic health record data to study variation in completion rates at the clinic and patient level of a remote MBC symptom measure tool during the first 6 months of implementation at three adult outpatient psychiatry clinics in a safety net health system. Provider-reported barriers to MBC adoption were also measured using repeated surveys at one of the three sites.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Out of 1219 patients who were sent an MBC measure request, uptake of completing at least one measure varied by clinic: General Adult Clinic, 38% (n = 262 of 696); Substance Use Clinic, 28% (n = 73 of 265); and Transitions Clinic, 17% (n = 44 of 258). Compared with White patients, Black and Portuguese or Brazilian patients had lower uptake. Older patients also had lower uptake. Spanish language of care was associated with much lower uptake at the patient level. Significant patient-level disparities in uptake persisted after adjusting for the clinic, mental health diagnoses, and number of measure requests sent. Providers cited time within visits and bandwidth in their workflow as the greatest consistent barriers to discussing MBC results with patients.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>There are significant disparities in MBC uptake at the patient and clinic level. From an LHS data infrastructure perspective, safety net health systems may need to address the need for possible ways to adapt MBC to better fit their populations and clinical needs, or identify targeted implementation strategies to close data gaps for the identified disparity populations.</p>\\n </section>\\n </div>\",\"PeriodicalId\":43916,\"journal\":{\"name\":\"Learning Health Systems\",\"volume\":\"8 S1\",\"pages\":\"\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-04-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10416\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Learning Health Systems\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10416\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Learning Health Systems","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10416","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
摘要
导言 基于行为测量的护理(MBC)可以改善患者的治疗效果,同时也被认为是一种重要的学习型医疗系统(LHS)工具,可用于识别和减少心理健康治疗中的潜在差异。然而,人们对安全网环境中远程行为 MBC 的采用情况,或远程 MBC 实施过程中可能出现的差异知之甚少。 方法 本研究使用电子健康记录数据,研究在安全网医疗系统的三家成人精神科门诊实施远程 MBC 症状测量工具的前 6 个月中,诊所和患者层面完成率的差异。此外,还在三家诊所中的一家进行了重复调查,以衡量医疗服务提供者报告的采用 MBC 的障碍。 结果 在收到 MBC 测量请求的 1219 名患者中,完成至少一项测量的比例因诊所而异:普通成人诊所,38%(696 人中有 262 人);药物使用诊所,28%(265 人中有 73 人);过渡诊所,17%(258 人中有 44 人)。与白人患者相比,黑人和葡萄牙或巴西籍患者的接受率较低。年龄较大的患者使用率也较低。在患者层面,使用西班牙语就医的比例要低得多。在对诊所、心理健康诊断和发出的测量请求数量进行调整后,患者层面的接受率仍存在显著差异。医疗服务提供者认为,就诊时间和工作流程带宽是与患者讨论 MBC 结果的最大障碍。 结论 在患者和诊所层面,MBC 的使用率存在显著差异。从长效医疗系统数据基础设施的角度来看,安全网医疗系统可能需要解决如何调整 MBC 以更好地适应其人群和临床需求的问题,或确定有针对性的实施策略,以缩小已确定的差异人群的数据差距。
Determinants of remote measurement-based care uptake in a safety net outpatient psychiatry department as part of learning health system transition
Introduction
Behavioral measurement-based care (MBC) can improve patient outcomes and has also been advanced as a critical learning health system (LHS) tool for identifying and mitigating potential disparities in mental health treatment. However, little is known about the uptake of remote behavioral MBC in safety net settings, or possible disparities occurring in remote MBC implementation.
Methods
This study uses electronic health record data to study variation in completion rates at the clinic and patient level of a remote MBC symptom measure tool during the first 6 months of implementation at three adult outpatient psychiatry clinics in a safety net health system. Provider-reported barriers to MBC adoption were also measured using repeated surveys at one of the three sites.
Results
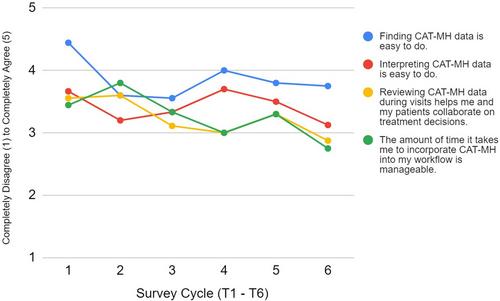
Out of 1219 patients who were sent an MBC measure request, uptake of completing at least one measure varied by clinic: General Adult Clinic, 38% (n = 262 of 696); Substance Use Clinic, 28% (n = 73 of 265); and Transitions Clinic, 17% (n = 44 of 258). Compared with White patients, Black and Portuguese or Brazilian patients had lower uptake. Older patients also had lower uptake. Spanish language of care was associated with much lower uptake at the patient level. Significant patient-level disparities in uptake persisted after adjusting for the clinic, mental health diagnoses, and number of measure requests sent. Providers cited time within visits and bandwidth in their workflow as the greatest consistent barriers to discussing MBC results with patients.
Conclusions
There are significant disparities in MBC uptake at the patient and clinic level. From an LHS data infrastructure perspective, safety net health systems may need to address the need for possible ways to adapt MBC to better fit their populations and clinical needs, or identify targeted implementation strategies to close data gaps for the identified disparity populations.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
