{"title":"假性低钾血症病例报告--血钾正常意味着什么?","authors":"Tomáš Šálek, David Stejskal","doi":"10.11613/BM.2024.021002","DOIUrl":null,"url":null,"abstract":"<p><p>This case report describes a case of pseudonormokalemia, true hypokalemia. Often, only laboratory values outside the normal range gain attention and false normal results are at risk of not being noticed. However, a disease state may be masked by another pathological process. Here, a 50-year old male was admitted to the Department of Internal Medicine due to sepsis from a dental infection. Initially, serum potassium measurement revealed a normal value of 4 mmol/L (reference interval 3.8-5.1 mmol/L). Thrombocyte number was above 500x10<sup>9</sup>/L. Due to our policy to recommend a repeated measurement of potassium in whole blood or heparin plasma if a patient has thrombocytosis, pseudonormokalemia was identified because the heparin plasma potassium value was only 2.9 mmol/L (reference interval 3.5-4.8 mmol/L). The physiological difference between serum and plasma concentration is no more than 0.3 mmol/L. In this case, potassium concentration were falsely elevated in the serum sample, probably caused by the high number of platelets releasing potassium during clotting. Interpretative comments in patients with thrombocytosis over 500x10<sup>9</sup>/L recommending plasma potassium measurement are helpful. The best way to eliminate pseudohyperkalemia and pseudonormokalemia phenomena caused by thrombocytosis is to completely change towards heparin plasma as the standard material.</p>","PeriodicalId":94370,"journal":{"name":"Biochemia medica","volume":"34 2","pages":"021002"},"PeriodicalIF":1.8000,"publicationDate":"2024-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11177651/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pseudonormokalemia case report - What does it mean to have normal blood potassium?\",\"authors\":\"Tomáš Šálek, David Stejskal\",\"doi\":\"10.11613/BM.2024.021002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>This case report describes a case of pseudonormokalemia, true hypokalemia. Often, only laboratory values outside the normal range gain attention and false normal results are at risk of not being noticed. However, a disease state may be masked by another pathological process. Here, a 50-year old male was admitted to the Department of Internal Medicine due to sepsis from a dental infection. Initially, serum potassium measurement revealed a normal value of 4 mmol/L (reference interval 3.8-5.1 mmol/L). Thrombocyte number was above 500x10<sup>9</sup>/L. Due to our policy to recommend a repeated measurement of potassium in whole blood or heparin plasma if a patient has thrombocytosis, pseudonormokalemia was identified because the heparin plasma potassium value was only 2.9 mmol/L (reference interval 3.5-4.8 mmol/L). The physiological difference between serum and plasma concentration is no more than 0.3 mmol/L. In this case, potassium concentration were falsely elevated in the serum sample, probably caused by the high number of platelets releasing potassium during clotting. Interpretative comments in patients with thrombocytosis over 500x10<sup>9</sup>/L recommending plasma potassium measurement are helpful. The best way to eliminate pseudohyperkalemia and pseudonormokalemia phenomena caused by thrombocytosis is to completely change towards heparin plasma as the standard material.</p>\",\"PeriodicalId\":94370,\"journal\":{\"name\":\"Biochemia medica\",\"volume\":\"34 2\",\"pages\":\"021002\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-06-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11177651/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biochemia medica\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.11613/BM.2024.021002\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biochemia medica","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.11613/BM.2024.021002","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Pseudonormokalemia case report - What does it mean to have normal blood potassium?
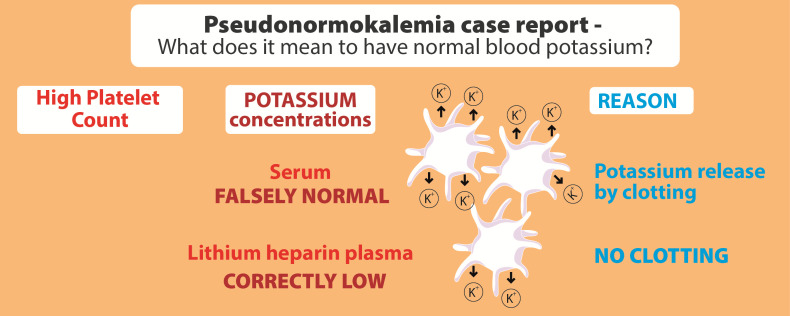
This case report describes a case of pseudonormokalemia, true hypokalemia. Often, only laboratory values outside the normal range gain attention and false normal results are at risk of not being noticed. However, a disease state may be masked by another pathological process. Here, a 50-year old male was admitted to the Department of Internal Medicine due to sepsis from a dental infection. Initially, serum potassium measurement revealed a normal value of 4 mmol/L (reference interval 3.8-5.1 mmol/L). Thrombocyte number was above 500x109/L. Due to our policy to recommend a repeated measurement of potassium in whole blood or heparin plasma if a patient has thrombocytosis, pseudonormokalemia was identified because the heparin plasma potassium value was only 2.9 mmol/L (reference interval 3.5-4.8 mmol/L). The physiological difference between serum and plasma concentration is no more than 0.3 mmol/L. In this case, potassium concentration were falsely elevated in the serum sample, probably caused by the high number of platelets releasing potassium during clotting. Interpretative comments in patients with thrombocytosis over 500x109/L recommending plasma potassium measurement are helpful. The best way to eliminate pseudohyperkalemia and pseudonormokalemia phenomena caused by thrombocytosis is to completely change towards heparin plasma as the standard material.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
