{"title":"ERAS 髋关节和膝关节置换术中贫血和缺铁情况的改善:描述性分析。","authors":"Christoffer Calov Jørgensen, Henrik Kehlet","doi":"10.1186/s13741-024-00426-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Preoperative anaemia including iron deficiency anaemia (IDA) is a well-established perioperative risk factor. However, most studies on iron therapy to treat IDA have been negative and few have been conducted within an enhanced recovery after surgery (ERAS) protocol. Furthermore, patients with IDA often have comorbidities not necessarily influenced by iron, but potentially influencing traditional study endpoints such as length of stay (LOS), morbidity, etc. The aim of this paper is to discuss patient-related challenges when planning outcome studies on the potential benefits of iron therapy in patients with IDA, based upon a large detailed prospective database in ERAS total hip (THA) and knee arthroplasty (TKA).</p><p><strong>Methods: </strong>A prospective observational cohort study in ERAS THA and TKA from 2022 to 2023. Detailed complete follow-up through questionnaires and electronic medical records.</p><p><strong>Results: </strong>Of 3655 included patients, 276 (7.6%) had IDA defined as a haemoglobin (Hb) of < 13.0 g/dL and transferrin saturation of 0.20, while 3379 had a Hb of ≥ 13.0. Patients with IDA were a median 5 years older than non-anaemics, with an increased fraction living alone (38.4% vs. 28.8%), using walking aids (54.3% vs 26.4%) and receiving home care (16.2% vs 4.7%). Fewer IDA patients were working (12.7% vs. 29.6%) and a median number of prescribed drugs was higher (10 vs. 6). Median LOS was 1 day in both IDA and non-anaemic patients, but a LOS of > 2 days occurred in 11.6% of patients with IDA vs. 4.3% in non-anaemics. The proportion with 30- or 90-day readmissions was 6.5% vs. 4.1% and. 13.4% vs6.0%, in patients with IDA and non-anaemics, respectively. However, potentially anaemia or iron deficiency-related causes of LOS > 2 days or 90-day readmissions were only 5.4% and 2.2% in patients with IDA and 1.9% and 1.0% in non-anaemics.</p><p><strong>Conclusion: </strong>Conventional randomised trials with single or composite \"hard\" endpoints are at risk of being inconclusive or underpowered due to a considerable burden of other patient-related risk factors and with postoperative complications which may not be modifiable by correction of IDA per se. We will propose to gain further insights from detailed observational and mechanistic studies prior to initiating extensive randomised studies.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"13 1","pages":"60"},"PeriodicalIF":2.1000,"publicationDate":"2024-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11193293/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcome improvement for anaemia and iron deficiency in ERAS hip and knee arthroplasty: a descriptive analysis.\",\"authors\":\"Christoffer Calov Jørgensen, Henrik Kehlet\",\"doi\":\"10.1186/s13741-024-00426-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>Preoperative anaemia including iron deficiency anaemia (IDA) is a well-established perioperative risk factor. However, most studies on iron therapy to treat IDA have been negative and few have been conducted within an enhanced recovery after surgery (ERAS) protocol. Furthermore, patients with IDA often have comorbidities not necessarily influenced by iron, but potentially influencing traditional study endpoints such as length of stay (LOS), morbidity, etc. The aim of this paper is to discuss patient-related challenges when planning outcome studies on the potential benefits of iron therapy in patients with IDA, based upon a large detailed prospective database in ERAS total hip (THA) and knee arthroplasty (TKA).</p><p><strong>Methods: </strong>A prospective observational cohort study in ERAS THA and TKA from 2022 to 2023. Detailed complete follow-up through questionnaires and electronic medical records.</p><p><strong>Results: </strong>Of 3655 included patients, 276 (7.6%) had IDA defined as a haemoglobin (Hb) of < 13.0 g/dL and transferrin saturation of 0.20, while 3379 had a Hb of ≥ 13.0. Patients with IDA were a median 5 years older than non-anaemics, with an increased fraction living alone (38.4% vs. 28.8%), using walking aids (54.3% vs 26.4%) and receiving home care (16.2% vs 4.7%). Fewer IDA patients were working (12.7% vs. 29.6%) and a median number of prescribed drugs was higher (10 vs. 6). Median LOS was 1 day in both IDA and non-anaemic patients, but a LOS of > 2 days occurred in 11.6% of patients with IDA vs. 4.3% in non-anaemics. The proportion with 30- or 90-day readmissions was 6.5% vs. 4.1% and. 13.4% vs6.0%, in patients with IDA and non-anaemics, respectively. However, potentially anaemia or iron deficiency-related causes of LOS > 2 days or 90-day readmissions were only 5.4% and 2.2% in patients with IDA and 1.9% and 1.0% in non-anaemics.</p><p><strong>Conclusion: </strong>Conventional randomised trials with single or composite \\\"hard\\\" endpoints are at risk of being inconclusive or underpowered due to a considerable burden of other patient-related risk factors and with postoperative complications which may not be modifiable by correction of IDA per se. We will propose to gain further insights from detailed observational and mechanistic studies prior to initiating extensive randomised studies.</p>\",\"PeriodicalId\":19764,\"journal\":{\"name\":\"Perioperative Medicine\",\"volume\":\"13 1\",\"pages\":\"60\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-06-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11193293/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Perioperative Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13741-024-00426-3\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-024-00426-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:包括缺铁性贫血(IDA)在内的术前贫血是公认的围手术期风险因素。然而,大多数有关铁疗法治疗 IDA 的研究结果都是负面的,很少有研究是在术后增强恢复(ERAS)方案中进行的。此外,IDA 患者通常有合并症,这些合并症并不一定受铁的影响,但有可能影响传统的研究终点,如住院时间(LOS)、发病率等。本文旨在根据 ERAS 全髋关节置换术(THA)和膝关节置换术(TKA)的大型详细前瞻性数据库,讨论在计划对 IDA 患者进行铁治疗的潜在益处的结果研究时,与患者相关的挑战:方法:对2022年至2023年ERAS全髋关节置换术(THA)和膝关节置换术(TKA)进行前瞻性队列观察研究。通过问卷调查和电子病历进行详细完整的随访:在纳入的 3655 名患者中,276 人(7.6%)患有 IDA,定义为血红蛋白(Hb)低于 2 天的 IDA 患者占 11.6%,非 IDA 患者占 4.3%。30 天或 90 天再入院的比例分别为 6.5% 对 4.1% 和 13.4% 对 6.0%。IDA患者和非贫血患者的30天或90天再入院比例分别为6.5%对4.1%和13.4%对6.0%。然而,与贫血或缺铁有关的导致住院时间超过2天或90天后再次入院的潜在原因,在IDA患者中分别仅为5.4%和2.2%,在非贫血患者中分别为1.9%和1.0%:结论:采用单一或复合 "硬 "终点的传统随机试验有可能无法得出结论,或由于与患者相关的其他风险因素和术后并发症的巨大负担而使试验能量不足,而这些并发症可能无法通过纠正IDA本身来改变。我们将建议在启动广泛的随机研究之前,从详细的观察性研究和机理研究中获得进一步的见解。
Outcome improvement for anaemia and iron deficiency in ERAS hip and knee arthroplasty: a descriptive analysis.
Background and purpose: Preoperative anaemia including iron deficiency anaemia (IDA) is a well-established perioperative risk factor. However, most studies on iron therapy to treat IDA have been negative and few have been conducted within an enhanced recovery after surgery (ERAS) protocol. Furthermore, patients with IDA often have comorbidities not necessarily influenced by iron, but potentially influencing traditional study endpoints such as length of stay (LOS), morbidity, etc. The aim of this paper is to discuss patient-related challenges when planning outcome studies on the potential benefits of iron therapy in patients with IDA, based upon a large detailed prospective database in ERAS total hip (THA) and knee arthroplasty (TKA).
Methods: A prospective observational cohort study in ERAS THA and TKA from 2022 to 2023. Detailed complete follow-up through questionnaires and electronic medical records.
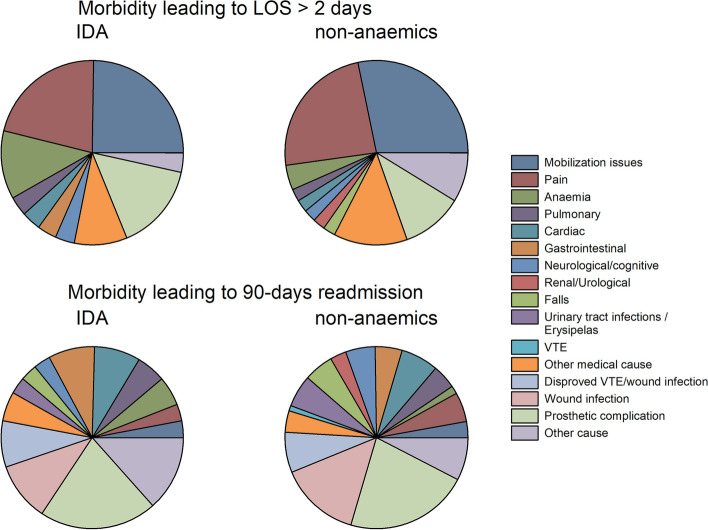
Results: Of 3655 included patients, 276 (7.6%) had IDA defined as a haemoglobin (Hb) of < 13.0 g/dL and transferrin saturation of 0.20, while 3379 had a Hb of ≥ 13.0. Patients with IDA were a median 5 years older than non-anaemics, with an increased fraction living alone (38.4% vs. 28.8%), using walking aids (54.3% vs 26.4%) and receiving home care (16.2% vs 4.7%). Fewer IDA patients were working (12.7% vs. 29.6%) and a median number of prescribed drugs was higher (10 vs. 6). Median LOS was 1 day in both IDA and non-anaemic patients, but a LOS of > 2 days occurred in 11.6% of patients with IDA vs. 4.3% in non-anaemics. The proportion with 30- or 90-day readmissions was 6.5% vs. 4.1% and. 13.4% vs6.0%, in patients with IDA and non-anaemics, respectively. However, potentially anaemia or iron deficiency-related causes of LOS > 2 days or 90-day readmissions were only 5.4% and 2.2% in patients with IDA and 1.9% and 1.0% in non-anaemics.
Conclusion: Conventional randomised trials with single or composite "hard" endpoints are at risk of being inconclusive or underpowered due to a considerable burden of other patient-related risk factors and with postoperative complications which may not be modifiable by correction of IDA per se. We will propose to gain further insights from detailed observational and mechanistic studies prior to initiating extensive randomised studies.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
