Rhiannon Nancarrow-Lei, Joana Hiew de Sousa Magalhães
{"title":"雾化高渗盐水治疗婴儿急性支气管炎。","authors":"Rhiannon Nancarrow-Lei, Joana Hiew de Sousa Magalhães","doi":"10.1111/cea.14530","DOIUrl":null,"url":null,"abstract":"<p>Acute bronchiolitis, marked by inflammation of the bronchioles, is characterised by airway oedema and mucus plugging resulting in wheeze [<span>1, 2</span>]. It is the most common lower respiratory tract infection in children aged less than 2 years, with Respiratory Syncytial Virus (RSV) being the most frequent cause [<span>1</span>]. Nebulised hypertonic saline solution (≥3%) may reduce these pathological changes and decrease airway obstruction, although the current available evidence is conflicting. This Cochrane Corner aims to assess the effects of nebulised hypertonic (≥3%) saline solution in infants with acute bronchiolitis.</p><p>Zhang L, Mendoza-Sassi RA, Wainwright CE, Aregbesola A, Klassen TP. Nebulised hypertonic saline solution for acute bronchiolitis in infants. <i>Cochrane Database of Syst Rev 2023</i>, Issue 3: CD006458.</p><p>Bronchiolitis is the leading cause of infant hospitalisation, largely secondary to lower respiratory tract infections, typically RSV [<span>1</span>]. In the UK, RSV results in 467,000 GP visits and 34,000 hospitalisations annually, with an estimated cost of £80 million for children under 5 [<span>4</span>]. The Joint Committee of Vaccination and Immunisation (JCVI) have recommended an RSV immunisation programme for infants and older adults, which will likely reshape the landscape of bronchiolitis [<span>5</span>].</p><p>Acute bronchiolitis, marked by airway oedema and mucus plugging, may benefit from nebulised hypertonic saline to aid airway secretion clearance. ‘Bronchiolitis’ encompasses a diverse group of conditions with varying underlying pathologies, emphasising the necessity for a validated diagnostic criteria, as highlighted in this Cochrane review.</p><p>This 2023 Cochrane review update of 34 trials involving 5205 infants, 2727 of whom received nebulised hypertonic saline. It found that nebulised hypertonic saline may result in a modest reduction in hospital stay length compared to treatment with nebulised normal saline or standard treatment. However, its impact on symptom resolution such as wheezing, cough, or pulmonary moist crackles, remains inconclusive. Nebulised hypertonic saline was linked to a lower risk of hospitalisation, but did not demonstrate a discernible reduction in re-admission rates. While hospital length of stay and hospitalisation rates are clinically important endpoints, they are potentially prone to bias. We support the Cochrane reviewers' call for a robust and universally accepted core outcome measures for infants with acute bronchiolitis.</p><p>Though the observed difference in effect size was smaller than that in the 2013 update, a nearly 10-h reduction in hospital stay may still hold clinical significance, given the disease's short natural course of 3–5 days. Though cost-effectiveness was not analysed, this reduction may lead to substantial cost savings. Challenges in drug delivery to crying infants and the use of normal saline as a control might have influenced negative findings [<span>6</span>].</p><p>The certainty of the evidence was generally graded as low to very low for all outcomes due to inconsistencies, high clinical heterogeneity, imprecision, and a risk of bias. Heterogeneity in nebulised hypertonic saline regimes (4–8 h) showed no statistical significance in subgroup analysis. Yet, more than two doses given to infants in outpatient and emergency departments conferred a greater effect size.</p><p>Reassuringly, no significant adverse effects were reported, most being mild and self-limiting, highlighting a good safety profile. Reported effects included worsening cough, agitation, bronchospasm, and vomiting and diarrhoea. Clinical trials are not always best placed to identify less common, severe adverse effects. Currently, the National Institute for Health and Care Excellence (NICE) does not recommend the use of hypertonic saline for the treatment of bronchiolitis in babies and children [<span>2</span>], likely due to the low or very low certainty of evidence.</p><p>In conclusion, nebulised hypertonic saline is a low-cost intervention with minimal known adverse effects. This Cochrane review demonstrates wide generalisability across various settings in high- and low-income countries. However, caution is required when extending these findings to infants with severe bronchiolitis, as most studies excluded this subgroup. Further research is warranted to assess the use of nebulised hypertonic saline in these cases.</p><p>Both authors contributed equally to this manuscript.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 8","pages":"534-537"},"PeriodicalIF":5.0000,"publicationDate":"2024-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14530","citationCount":"0","resultStr":"{\"title\":\"Nebulised Hypertonic Saline Solution for Acute Bronchiolitis in Infants\",\"authors\":\"Rhiannon Nancarrow-Lei, Joana Hiew de Sousa Magalhães\",\"doi\":\"10.1111/cea.14530\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Acute bronchiolitis, marked by inflammation of the bronchioles, is characterised by airway oedema and mucus plugging resulting in wheeze [<span>1, 2</span>]. It is the most common lower respiratory tract infection in children aged less than 2 years, with Respiratory Syncytial Virus (RSV) being the most frequent cause [<span>1</span>]. Nebulised hypertonic saline solution (≥3%) may reduce these pathological changes and decrease airway obstruction, although the current available evidence is conflicting. This Cochrane Corner aims to assess the effects of nebulised hypertonic (≥3%) saline solution in infants with acute bronchiolitis.</p><p>Zhang L, Mendoza-Sassi RA, Wainwright CE, Aregbesola A, Klassen TP. Nebulised hypertonic saline solution for acute bronchiolitis in infants. <i>Cochrane Database of Syst Rev 2023</i>, Issue 3: CD006458.</p><p>Bronchiolitis is the leading cause of infant hospitalisation, largely secondary to lower respiratory tract infections, typically RSV [<span>1</span>]. In the UK, RSV results in 467,000 GP visits and 34,000 hospitalisations annually, with an estimated cost of £80 million for children under 5 [<span>4</span>]. The Joint Committee of Vaccination and Immunisation (JCVI) have recommended an RSV immunisation programme for infants and older adults, which will likely reshape the landscape of bronchiolitis [<span>5</span>].</p><p>Acute bronchiolitis, marked by airway oedema and mucus plugging, may benefit from nebulised hypertonic saline to aid airway secretion clearance. ‘Bronchiolitis’ encompasses a diverse group of conditions with varying underlying pathologies, emphasising the necessity for a validated diagnostic criteria, as highlighted in this Cochrane review.</p><p>This 2023 Cochrane review update of 34 trials involving 5205 infants, 2727 of whom received nebulised hypertonic saline. It found that nebulised hypertonic saline may result in a modest reduction in hospital stay length compared to treatment with nebulised normal saline or standard treatment. However, its impact on symptom resolution such as wheezing, cough, or pulmonary moist crackles, remains inconclusive. Nebulised hypertonic saline was linked to a lower risk of hospitalisation, but did not demonstrate a discernible reduction in re-admission rates. While hospital length of stay and hospitalisation rates are clinically important endpoints, they are potentially prone to bias. We support the Cochrane reviewers' call for a robust and universally accepted core outcome measures for infants with acute bronchiolitis.</p><p>Though the observed difference in effect size was smaller than that in the 2013 update, a nearly 10-h reduction in hospital stay may still hold clinical significance, given the disease's short natural course of 3–5 days. Though cost-effectiveness was not analysed, this reduction may lead to substantial cost savings. Challenges in drug delivery to crying infants and the use of normal saline as a control might have influenced negative findings [<span>6</span>].</p><p>The certainty of the evidence was generally graded as low to very low for all outcomes due to inconsistencies, high clinical heterogeneity, imprecision, and a risk of bias. Heterogeneity in nebulised hypertonic saline regimes (4–8 h) showed no statistical significance in subgroup analysis. Yet, more than two doses given to infants in outpatient and emergency departments conferred a greater effect size.</p><p>Reassuringly, no significant adverse effects were reported, most being mild and self-limiting, highlighting a good safety profile. Reported effects included worsening cough, agitation, bronchospasm, and vomiting and diarrhoea. Clinical trials are not always best placed to identify less common, severe adverse effects. Currently, the National Institute for Health and Care Excellence (NICE) does not recommend the use of hypertonic saline for the treatment of bronchiolitis in babies and children [<span>2</span>], likely due to the low or very low certainty of evidence.</p><p>In conclusion, nebulised hypertonic saline is a low-cost intervention with minimal known adverse effects. This Cochrane review demonstrates wide generalisability across various settings in high- and low-income countries. However, caution is required when extending these findings to infants with severe bronchiolitis, as most studies excluded this subgroup. Further research is warranted to assess the use of nebulised hypertonic saline in these cases.</p><p>Both authors contributed equally to this manuscript.</p><p>The authors declare no conflicts of interest.</p>\",\"PeriodicalId\":10207,\"journal\":{\"name\":\"Clinical and Experimental Allergy\",\"volume\":\"54 8\",\"pages\":\"534-537\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-06-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14530\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cea.14530\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14530","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
Nebulised Hypertonic Saline Solution for Acute Bronchiolitis in Infants
Acute bronchiolitis, marked by inflammation of the bronchioles, is characterised by airway oedema and mucus plugging resulting in wheeze [1, 2]. It is the most common lower respiratory tract infection in children aged less than 2 years, with Respiratory Syncytial Virus (RSV) being the most frequent cause [1]. Nebulised hypertonic saline solution (≥3%) may reduce these pathological changes and decrease airway obstruction, although the current available evidence is conflicting. This Cochrane Corner aims to assess the effects of nebulised hypertonic (≥3%) saline solution in infants with acute bronchiolitis.
Zhang L, Mendoza-Sassi RA, Wainwright CE, Aregbesola A, Klassen TP. Nebulised hypertonic saline solution for acute bronchiolitis in infants. Cochrane Database of Syst Rev 2023, Issue 3: CD006458.
Bronchiolitis is the leading cause of infant hospitalisation, largely secondary to lower respiratory tract infections, typically RSV [1]. In the UK, RSV results in 467,000 GP visits and 34,000 hospitalisations annually, with an estimated cost of £80 million for children under 5 [4]. The Joint Committee of Vaccination and Immunisation (JCVI) have recommended an RSV immunisation programme for infants and older adults, which will likely reshape the landscape of bronchiolitis [5].
Acute bronchiolitis, marked by airway oedema and mucus plugging, may benefit from nebulised hypertonic saline to aid airway secretion clearance. ‘Bronchiolitis’ encompasses a diverse group of conditions with varying underlying pathologies, emphasising the necessity for a validated diagnostic criteria, as highlighted in this Cochrane review.
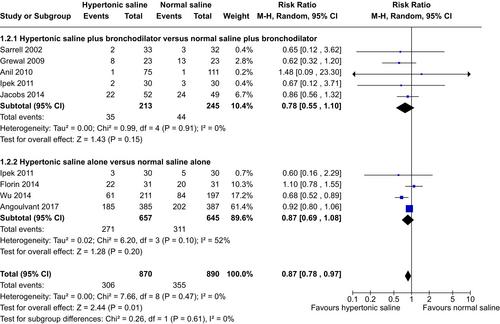
This 2023 Cochrane review update of 34 trials involving 5205 infants, 2727 of whom received nebulised hypertonic saline. It found that nebulised hypertonic saline may result in a modest reduction in hospital stay length compared to treatment with nebulised normal saline or standard treatment. However, its impact on symptom resolution such as wheezing, cough, or pulmonary moist crackles, remains inconclusive. Nebulised hypertonic saline was linked to a lower risk of hospitalisation, but did not demonstrate a discernible reduction in re-admission rates. While hospital length of stay and hospitalisation rates are clinically important endpoints, they are potentially prone to bias. We support the Cochrane reviewers' call for a robust and universally accepted core outcome measures for infants with acute bronchiolitis.
Though the observed difference in effect size was smaller than that in the 2013 update, a nearly 10-h reduction in hospital stay may still hold clinical significance, given the disease's short natural course of 3–5 days. Though cost-effectiveness was not analysed, this reduction may lead to substantial cost savings. Challenges in drug delivery to crying infants and the use of normal saline as a control might have influenced negative findings [6].
The certainty of the evidence was generally graded as low to very low for all outcomes due to inconsistencies, high clinical heterogeneity, imprecision, and a risk of bias. Heterogeneity in nebulised hypertonic saline regimes (4–8 h) showed no statistical significance in subgroup analysis. Yet, more than two doses given to infants in outpatient and emergency departments conferred a greater effect size.
Reassuringly, no significant adverse effects were reported, most being mild and self-limiting, highlighting a good safety profile. Reported effects included worsening cough, agitation, bronchospasm, and vomiting and diarrhoea. Clinical trials are not always best placed to identify less common, severe adverse effects. Currently, the National Institute for Health and Care Excellence (NICE) does not recommend the use of hypertonic saline for the treatment of bronchiolitis in babies and children [2], likely due to the low or very low certainty of evidence.
In conclusion, nebulised hypertonic saline is a low-cost intervention with minimal known adverse effects. This Cochrane review demonstrates wide generalisability across various settings in high- and low-income countries. However, caution is required when extending these findings to infants with severe bronchiolitis, as most studies excluded this subgroup. Further research is warranted to assess the use of nebulised hypertonic saline in these cases.
Both authors contributed equally to this manuscript.
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
