T. Buttgereit, F. Aulenbacher, A. Gutsche, P. Kolkhir, K. Weller, C. Vera Ayala, M. Magerl, H. Farkas, A. S. Grumach, E. Aygören-Pürsün, N. Bara, M. Ben-Shoshan, J. Bernstein, S. Betschel, L. Bouillet, T. Caballero, M. Cancian, A. J. Castaldo, S. Cimbollek, D. M. Cohn, T. Craig, D. Fomina, A. Gelincik, V. Grivcheva-Panovska, A. Jindal, C. Katelaris, A. Kessel, T. Kinaciyan, H. J. Longhurst, I. Martinez-Saguer, M. Riedl, C. Schöffl, P. Staubach, A. Zanichelli, Y. Zhi, H. Balle Boysen, J. S. Fok, P. H. Li, R. Hakl, M. Hide, J. Peter, M. Maurer
{"title":"慢性血管性水肿登记处(CARE):原理、方法和实施。","authors":"T. Buttgereit, F. Aulenbacher, A. Gutsche, P. Kolkhir, K. Weller, C. Vera Ayala, M. Magerl, H. Farkas, A. S. Grumach, E. Aygören-Pürsün, N. Bara, M. Ben-Shoshan, J. Bernstein, S. Betschel, L. Bouillet, T. Caballero, M. Cancian, A. J. Castaldo, S. Cimbollek, D. M. Cohn, T. Craig, D. Fomina, A. Gelincik, V. Grivcheva-Panovska, A. Jindal, C. Katelaris, A. Kessel, T. Kinaciyan, H. J. Longhurst, I. Martinez-Saguer, M. Riedl, C. Schöffl, P. Staubach, A. Zanichelli, Y. Zhi, H. Balle Boysen, J. S. Fok, P. H. Li, R. Hakl, M. Hide, J. Peter, M. Maurer","doi":"10.1111/cea.14527","DOIUrl":null,"url":null,"abstract":"<p>Angioedema (AE) is a paroxysmal, localised and self-limiting swelling of the subcutaneous and/or submucosal tissue, because of a temporary increase in vascular permeability. Recurrent AE is a heterogeneous disease, which is categorised into different types [<span>1</span>]. Clinical and sociodemographic core factors in AE remain insufficiently investigated. A need exists for a large, comprehensive worldwide registry for all types of recurrent AE, applying modern methodologies and parameters from recent scientific knowledge.</p><p>Chronic Angioedema Registry (CARE) is an international, prospective, multicentre, observational (noninterventional), open-ended disease registry initiated in 2023 by the global network of Angioedema Centers of Reference and Excellence (ACARE) and the Urticaria Network e.V. (UNEV), which aims to enhance the understanding of recurrent AE of all aetiologies in worldwide clinical settings.</p><p>All physicians treating patients with AE, irrespective of location, medical specialty or setting, are invited to participate in CARE. The requirements for participation and the ‘Project Plan’ and ‘CARE Charter’ can be found on the CARE website (https://chronic-angioedema-registry.com). Participation in CARE incurs no costs, no financial compensation or support is provided, and no charges will be billed to health insurers. Data submission is voluntary and solely at the physician and patient's discretion.</p><p>The CARE questionnaires, developed by the CARE International Steering Committee (ISC), consist of basic multiple-choice or short-answer questions. Questions and variables are programmed in REDCap (Nashville, Tennessee), a secure, web-based software platform designed to support data capture for research studies (https://www.project-redcap.org; downloaded on 5 July 2023). After giving their written informed consent, participating patients receive a QR code linked to their participant identification (ID) number, allowing them to access the patient questionnaire via a smart device; the treating physician gets the patient's ID and completes the physician questionnaire (Figure 1).</p><p>CARE data will be collected during routine patient consultation visits and examinations for AE treatment. CARE will continue to follow patients as long as the physician and patient are considered appropriate. Data will be transferred at regular periods from REDCap into an electronic case report form programme to process and monitor the data. Outlier and diagnostic plots are used to check for plausibility, consistency and integrity.</p><p>The registry database is owned, hosted and administered by UNEV. Participating physicians are responsible for retaining all source data, and the staff of the treating physician must monitor and manage the patient's data. If patients withdraw their consent, their data will not be further included. A patient's previous data will be deleted from the registry upon a patient's request.</p><p>Patient baseline and follow-up questionnaires can be completed within 20 and 15 min, respectively, and are developed in different languages. Both questionnaires contain pictures and descriptions of AE and wheals to ensure patients comprehend the distinctions. Baseline questionnaires collect data on patient's demographics, disease duration, disease course, frequency, underlying causes, comorbidities, triggering factors, treatments, disease activity, disease control, quality of life impairment and direct healthcare costs. Follow-up questionnaires gather data about changes in the patient's signs and symptoms, disease control, quality of life, treatments and healthcare usage. No time point for follow-up data collection is specified, but this should occur between 3 months and 1 year. In both patient questionnaires, the Angioedema Control Test and the Angioedema Quality of Life Questionnaire are used to assess disease control and disease-related quality of life, respectively [<span>2, 3</span>]. In the physician baseline and follow-up questionnaires, the treating physician reports the type of AE.</p><p>Participating physicians may analyse and publish CARE data. They can obtain a spreadsheet of raw data by submitting a ‘Request for Analysis’ to UNEV. The CARE ISC will help manage publications, and the proposing physician will lead the group of coauthors. Physicians retain the right to independently analyse, present and publish their data without seeking approval from the CARE ISC, but their publications must acknowledge the CARE project's contributions.</p><p>CARE is subjected to the typical limitations that apply to observational studies and specific constraints associated with registries. Many participating physicians/sites have specialised AE expertise, leading to a likelihood that enrolled patients have more complex conditions and severe forms. Consequently, the outcomes derived from CARE may not broadly apply to less severe cases of AE typically seen in primary care or community settings. In addition, participating physicians are not obligated to continuously register all AE patients, leading to an unintended selection bias. Furthermore, the findings may not always be generalisable to patients globally or those from diverse ethnic backgrounds.</p><p>Although a few international and national registries on AE have been previously initiated, they had relatively small patient numbers, assessed a limited number of parameters and exclusively focussed on either hereditary angioedema or chronic urticaria [<span>4-6</span>]. Because of its large patient size, CARE has the potential to detect and assess even rare forms of AE and to elicit treatment responses. In future, CARE will benefit from joint analyses with other registries, such as the Chronic Urticaria Registry, as further assessments of the overlap between different AE types could better understand disease phenotypes, link pathogenic drivers and guide patient care [<span>5, 7, 8</span>]. Additionally, once CARE data start being recorded, it could be linked to currently used patient apps such as CRUSE, a patient app used to monitor and control chronic urticaria, or to patient biobank blood samples [<span>9</span>].</p><p>In conclusion, CARE could become the most modern, comprehensive research project on recurrent AE of all aetiologies. Collecting real-life data in CARE will equip physicians and researchers with better information on managing, monitoring and improving patient care in AE.</p><p>T. Buttgereit, F. Aulenbacher, A. Gutsche, M. Maurer, M. Magerl and K. Weller designed the study with input from all authors. T. Buttgereit and M. Maurer prepared the main manuscript text. All authors contributed to writing or reviewing the manuscript and final approval.</p><p>T. Buttgereit is or recently was a speaker and/or advisor for Aquestive, AstraZeneca, Biocryst, CSL-Behring, GlaxoSmithKline, Hexal, KalVista, Medac, Novartis, Pharming, Pharvaris, Roche, Sanofi, Swixx BioPharma and Takeda. P. Kolkhir has been a speaker for Novartis, ValenzaBio and Roche. A. Gutsche has no conflicts of interest in relation to this work. F. Aulenbacher has no conflicts of interest in relation to this work. K. Weller has no conflicts of interest in relation to this work. Outside it, he is or recently was a speaker and/or advisor for and/or has received research funding from Biocryst, CSL-Behring, Moxie, Novartis, Sanofi and Takeda. C. Vera Ayala has no conflicts of interest in relation to this work. M. Magerl is or recently was a speaker and/or advisor for and/or has received research funding from Biocryst, Pharming, Takeda, CSL Behring, Ionis Pharmaceuticals, KalVista and Pharvaris. H. Farkas has no conflicts of interest in relation to this work. Outside it, she has received research grants from CSL Behring, Takeda and Pharming. She was a speaker and/or advisor for CSL Behring, Takeda, Pharming KalVista, ONO Pharmaceutical, Pharvaris, Astria, Intellia and Biocryst. A. S. Grumach has no conflicts of interest in relation to this work. She has received a grant from the Brazilian National Council of Research (CNPq) and Takeda and is or recently was a speaker and/or advisor for Takeda, CSL-Behring, Pharvaris, KalVista, Exeltis, Pint-Pharma, Biomarin, Binding site and Multicare. E. Aygören-Pürsün has received grants from CSL Behring and Takeda and consulting fees from CSL Behring, Biocryst, KalVista and Pharvaris. He has received speaker fees from CSL Behring, Biocryst, Centogene, Pharming and Takeda and has received fees as an advisor for Astria, Biocryst, BioMarin Europe, Centogene, CSL Behring, Intellia, KalVista, Pharming, Pharvaris and Takeda. N. Bara has received grants from Takeda and has received payment for lectures/presentations from Takeda, Pharming and CSL Behring. She has participated in advisory boards for Takeda, Pharming, KalVista and Biocryst and has participated in a committee or advocacy group for the Romanian Registry for the HAE Foundation, the Roman Society of Allergy and Clinical Immunology and is head of the Romanian Expert Committee for Hereditary Angioedema. M. Ben-Shoshan is or recently was a speaker and/or advisor for Sanofi and Novartis. J. Bernstein has received grants from Takeda/Shire, CSL Behring, Pharming, Biocryst, Biomarin, Ionis Pharmaceuticals, KalVista, Sanofi, Regeneron, Astra Zeneca, Amgen, Novartis, Genentech, Celldex, Jasper, Escient, Allakos, Blueprint Medicine, Cogent, Telios, Astria and Teva. He has received consulting fees from Pharvaris and is the president of AAAAI. S. Betschel has received payment for lectures/presentations from Biocryst, CSL Behring, KalVista and Takeda and has received travel support from Biocryst, CSL Behring, KalVista and Takeda. He has participated in advisory boards for Ionis Pharmaceuticals, Pharvaris, Takeda, CSL Behring, Novartis, Astria and Biocryst. He is the voluntary chair of the Canadian Hereditary Angioedema Network. L. Bouillet has received consulting fees and has received payment or honoraria from CSL Behring, Takeda, Biocryst, Pharvaris, Novartis and GlaxoSmithKline. He has attended meetings for CSL Behring, Takeda, Biocryst, Novartis and GlaxoSmithKline and has participated in advisory boards for CSL Behring, Takeda, Biocryst, Pharvaris, Intellia and KalVista. He is in a leadership position for the SNFMI (French Internal Medicine Society). T. Caballero has no conflicts of interest in relation to this work. Outside it, she has participated in advisory boards for Astria, Biocryst, CSL Behring, KalVista, Novartis, Pharming, Pharvaris and Takeda. She is a member of speaker bureaus for Biocryst, CSL Behring, Novartis, Pharming and Takeda and has received grants from CSL Behring and Takeda. She has received funding to attend conferences/educational events from Biocryst, CSL Behring, Novartis, Pharming and Takeda and is/has been a clinical trial/registry investigator for Biocryst, CSL Behring, Ionis Pharmaceuticals, KalVista, Novartis, Pharming and Takeda. She is a researcher from the IdiPAZ programme for promoting research activities. M. Cancian has received personal fees from Biocryst, CSL Behring, KalVista and Takeda. A. J. Castaldo has no conflicts of interest. S. Cimbollek was a speaker and/or advisor for and/or received research funding from Takeda, Novartis, Pharming, CSL Behring, Biocryst, GlaxoSmithKline, Sanofi/Regeneron and Astra Zeneca. D. M. Cohn has received speaking fees from CSL Behring, Ionis Pharmaceuticals, Pharvaris and Takeda and consultancy fees from Astria, Biocryst, CSL Behring, Ionis Pharmaceuticals, KalVista, Pharming, Pharvaris and Takeda. He has received research support from Ionis Pharmaceuticals, KalVista, Pharvaris and Takeda. T. Craig has served as a speaker and researcher for Biomarin, CSL Behring, Intellia and Takeda and has been a researcher for Astria, Ionis Pharmaceuticals, KalVista and Pharvaris. He has been a speaker for Grifols and a consultant for Astria, Biocryst, Biomarin, CSL Behring, Intellia and Spark. He is the director of ACARE International Hereditary Angioedema Center and a member of the Medical Advisory Board for the HAE-A. D. Fomina has no conflicts in relation to this work. A. Gelincik is or recently was a speaker and/or advisor for Takeda and Pharvaris and has received research funding from Ionis Pharmaceuticals, Takeda and Pharvaris. V. Grivcheva-Panovska has received travel support from Pharming and Takeda. A. Jindal has no conflicts of interest in relation to this work. C. Katelaris has received institutional funding as a Principal Investigator on clinical trials for CSL Behring, KVD Pharma, Intellia and Biocryst and has received payments for presentations and advisory board participation from CSL Behring, Takeda, Phavaris, KVD Pharma, GlaxoSmithKline, Menarini, Novartis and Sanofi. A. Kessel has received consulting fees from Biocryst, KalVista and Takeda and has received payment for lectures/presentations from Takeda. He has received travel support from Takeda and has participated in advisory boards for KalVista and Takeda. He has received equipment or services from Takeda. T. Kinaciyan is or recently was a speaker and/or advisor for and/or has received research funding from Biocryst, CSL Behring, KalVista Pharmaceuticals, Pharming, Pharvaris, Sanofi and Takeda. H. Longhurst is or recently was a speaker and/or advisor for and/or has received research funding from CSL Behring, Intellia, KalVista, Pharming and Takeda I. Martinez-Saguer is recently or was a speaker and/or advisor for and/or has received research funding from Biocryst, CSL Behring, KalVista, Pharming, Pharvaris, Octapharma and Takeda. M. Riedl has received research grants from Biocryst, Biomarin, CSL Behring, Ionis Pharmaceuticals, KalVista, Pharvaris and Takeda and has served as a consultant for Astria, Biocryst, Biomarin, Celldex, CSL Behring, Cycle Pharma, Grifols, Intellia, KalVista, Pfizer, Pharming, Pharvaris, Sanofi-Regeneron and Takeda. C. Schöffl has received payment for lectures/presentations from Biocryst, CSL Behring, KalVista and Takeda and has received travel support from Biocryst, CSL Behring and Takeda. He has participated in advisory boards for Biocryst, CSL Behring, KalVista and Takeda and is a board member of the Austrian HAE member organisation. P. Staubach has no conflicts in relation to this work. Outside it, she has received grants from Novartis and Sanofi and has received consulting fees from CSL Behring, Octapharma, Novartis, Biocryst, Takeda, Sanofi/Regeneron and Genzyme. She is a member of the Society of Dermopharmazie. A. Zanichelli has received honoraria as a speaker/advisor from Biocryst, CSL Behring, KalVista, Pharming, Pharvaris and Takeda. Y-X. Zhi has no conflicts of interest in relation to this work. H. B. Boysen has no conflicts of interest in relation to this work. Jie Shen Fok has received payments for lectures/presentations from Viatris, Novartis, CSL Behring and Takeda and has received travel support from Viatris, CSL Behring and Takeda. Philip Li has no conflicts in relation to this work. R. Hakl has no conflicts of interest in relation to this work. Outside it, he has received consultancy/speaker honoraria from CSL Behring, Shire and Takeda and has served as a principal investigator for clinical trials sponsored by Biocryst, Pharvaris, Pharming, CSL Behring and KalVista. M. Hide is or recently was a speaker and/or advisor for CSL Behring, Eisai, Kaken, KalVista, Kyorin, Kyowa-Kirin, Meiji, Mitsubishi Tanabe Pharma, Nippon Zoki, Novartis, Pharvaris, Sanofi/Regeneron, Taiho, Takeda, Teikoku and Torii. J. Peter is or recently was a speaker and/or advisor for and/or has received research funding from Abbivie, AstraZeneca, Astria, Biocryst, CSL Behring, GlaxoSmithKline, Glenmark, KalVista, Novartis, Pharvaris, Sanofi/Regeneron, Takeda and Johnson & Johnson. M. Maurer is or recently was a speaker and/or advisor for and/or has received research funding from Allakos, Alvotech, Amgen, Aquestive, Aralez, AstraZeneca, Astria, Bayer, Biocryst, Blueprint, Celldex, Celltrion, Centogene, CSL Behring, Evommune, GlaxoSmithKline, Ipsen, KalVista, Kyowa Kirin, Leo Pharma, Lilly, Menarini, Mitsubishi Tanabe Pharma, Moxie, Noucor, Novartis, Orion Biotechnology, Pharvaris, Resonance Medicine, Sanofi/Regeneron, Septerna, Takeda, Teva, Third HarmonicBio, Valenza Bio, Yuhan Corporation and Zurabio.</p><p>The CARE study received initial approval in August 2023 from the Ethics Committee of Charité—Universitätsmedizin Berlin (reference no.: EA2/145/23). All other participating institutions must obtain approval from their respective ethics committees as required by national laws before being included in the registry.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 9","pages":"712-716"},"PeriodicalIF":5.0000,"publicationDate":"2024-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14527","citationCount":"0","resultStr":"{\"title\":\"The Chronic Angioedema Registry (CARE): Rationale, Methods and Implementation\",\"authors\":\"T. Buttgereit, F. Aulenbacher, A. Gutsche, P. Kolkhir, K. Weller, C. Vera Ayala, M. Magerl, H. Farkas, A. S. Grumach, E. Aygören-Pürsün, N. Bara, M. Ben-Shoshan, J. Bernstein, S. Betschel, L. Bouillet, T. Caballero, M. Cancian, A. J. Castaldo, S. Cimbollek, D. M. Cohn, T. Craig, D. Fomina, A. Gelincik, V. Grivcheva-Panovska, A. Jindal, C. Katelaris, A. Kessel, T. Kinaciyan, H. J. Longhurst, I. Martinez-Saguer, M. Riedl, C. Schöffl, P. Staubach, A. Zanichelli, Y. Zhi, H. Balle Boysen, J. S. Fok, P. H. Li, R. Hakl, M. Hide, J. Peter, M. Maurer\",\"doi\":\"10.1111/cea.14527\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Angioedema (AE) is a paroxysmal, localised and self-limiting swelling of the subcutaneous and/or submucosal tissue, because of a temporary increase in vascular permeability. Recurrent AE is a heterogeneous disease, which is categorised into different types [<span>1</span>]. Clinical and sociodemographic core factors in AE remain insufficiently investigated. A need exists for a large, comprehensive worldwide registry for all types of recurrent AE, applying modern methodologies and parameters from recent scientific knowledge.</p><p>Chronic Angioedema Registry (CARE) is an international, prospective, multicentre, observational (noninterventional), open-ended disease registry initiated in 2023 by the global network of Angioedema Centers of Reference and Excellence (ACARE) and the Urticaria Network e.V. (UNEV), which aims to enhance the understanding of recurrent AE of all aetiologies in worldwide clinical settings.</p><p>All physicians treating patients with AE, irrespective of location, medical specialty or setting, are invited to participate in CARE. The requirements for participation and the ‘Project Plan’ and ‘CARE Charter’ can be found on the CARE website (https://chronic-angioedema-registry.com). Participation in CARE incurs no costs, no financial compensation or support is provided, and no charges will be billed to health insurers. Data submission is voluntary and solely at the physician and patient's discretion.</p><p>The CARE questionnaires, developed by the CARE International Steering Committee (ISC), consist of basic multiple-choice or short-answer questions. Questions and variables are programmed in REDCap (Nashville, Tennessee), a secure, web-based software platform designed to support data capture for research studies (https://www.project-redcap.org; downloaded on 5 July 2023). After giving their written informed consent, participating patients receive a QR code linked to their participant identification (ID) number, allowing them to access the patient questionnaire via a smart device; the treating physician gets the patient's ID and completes the physician questionnaire (Figure 1).</p><p>CARE data will be collected during routine patient consultation visits and examinations for AE treatment. CARE will continue to follow patients as long as the physician and patient are considered appropriate. Data will be transferred at regular periods from REDCap into an electronic case report form programme to process and monitor the data. Outlier and diagnostic plots are used to check for plausibility, consistency and integrity.</p><p>The registry database is owned, hosted and administered by UNEV. Participating physicians are responsible for retaining all source data, and the staff of the treating physician must monitor and manage the patient's data. If patients withdraw their consent, their data will not be further included. A patient's previous data will be deleted from the registry upon a patient's request.</p><p>Patient baseline and follow-up questionnaires can be completed within 20 and 15 min, respectively, and are developed in different languages. Both questionnaires contain pictures and descriptions of AE and wheals to ensure patients comprehend the distinctions. Baseline questionnaires collect data on patient's demographics, disease duration, disease course, frequency, underlying causes, comorbidities, triggering factors, treatments, disease activity, disease control, quality of life impairment and direct healthcare costs. Follow-up questionnaires gather data about changes in the patient's signs and symptoms, disease control, quality of life, treatments and healthcare usage. No time point for follow-up data collection is specified, but this should occur between 3 months and 1 year. In both patient questionnaires, the Angioedema Control Test and the Angioedema Quality of Life Questionnaire are used to assess disease control and disease-related quality of life, respectively [<span>2, 3</span>]. In the physician baseline and follow-up questionnaires, the treating physician reports the type of AE.</p><p>Participating physicians may analyse and publish CARE data. They can obtain a spreadsheet of raw data by submitting a ‘Request for Analysis’ to UNEV. The CARE ISC will help manage publications, and the proposing physician will lead the group of coauthors. Physicians retain the right to independently analyse, present and publish their data without seeking approval from the CARE ISC, but their publications must acknowledge the CARE project's contributions.</p><p>CARE is subjected to the typical limitations that apply to observational studies and specific constraints associated with registries. Many participating physicians/sites have specialised AE expertise, leading to a likelihood that enrolled patients have more complex conditions and severe forms. Consequently, the outcomes derived from CARE may not broadly apply to less severe cases of AE typically seen in primary care or community settings. In addition, participating physicians are not obligated to continuously register all AE patients, leading to an unintended selection bias. Furthermore, the findings may not always be generalisable to patients globally or those from diverse ethnic backgrounds.</p><p>Although a few international and national registries on AE have been previously initiated, they had relatively small patient numbers, assessed a limited number of parameters and exclusively focussed on either hereditary angioedema or chronic urticaria [<span>4-6</span>]. Because of its large patient size, CARE has the potential to detect and assess even rare forms of AE and to elicit treatment responses. In future, CARE will benefit from joint analyses with other registries, such as the Chronic Urticaria Registry, as further assessments of the overlap between different AE types could better understand disease phenotypes, link pathogenic drivers and guide patient care [<span>5, 7, 8</span>]. Additionally, once CARE data start being recorded, it could be linked to currently used patient apps such as CRUSE, a patient app used to monitor and control chronic urticaria, or to patient biobank blood samples [<span>9</span>].</p><p>In conclusion, CARE could become the most modern, comprehensive research project on recurrent AE of all aetiologies. Collecting real-life data in CARE will equip physicians and researchers with better information on managing, monitoring and improving patient care in AE.</p><p>T. Buttgereit, F. Aulenbacher, A. Gutsche, M. Maurer, M. Magerl and K. Weller designed the study with input from all authors. T. Buttgereit and M. Maurer prepared the main manuscript text. All authors contributed to writing or reviewing the manuscript and final approval.</p><p>T. Buttgereit is or recently was a speaker and/or advisor for Aquestive, AstraZeneca, Biocryst, CSL-Behring, GlaxoSmithKline, Hexal, KalVista, Medac, Novartis, Pharming, Pharvaris, Roche, Sanofi, Swixx BioPharma and Takeda. P. Kolkhir has been a speaker for Novartis, ValenzaBio and Roche. A. Gutsche has no conflicts of interest in relation to this work. F. Aulenbacher has no conflicts of interest in relation to this work. K. Weller has no conflicts of interest in relation to this work. Outside it, he is or recently was a speaker and/or advisor for and/or has received research funding from Biocryst, CSL-Behring, Moxie, Novartis, Sanofi and Takeda. C. Vera Ayala has no conflicts of interest in relation to this work. M. Magerl is or recently was a speaker and/or advisor for and/or has received research funding from Biocryst, Pharming, Takeda, CSL Behring, Ionis Pharmaceuticals, KalVista and Pharvaris. H. Farkas has no conflicts of interest in relation to this work. Outside it, she has received research grants from CSL Behring, Takeda and Pharming. She was a speaker and/or advisor for CSL Behring, Takeda, Pharming KalVista, ONO Pharmaceutical, Pharvaris, Astria, Intellia and Biocryst. A. S. Grumach has no conflicts of interest in relation to this work. She has received a grant from the Brazilian National Council of Research (CNPq) and Takeda and is or recently was a speaker and/or advisor for Takeda, CSL-Behring, Pharvaris, KalVista, Exeltis, Pint-Pharma, Biomarin, Binding site and Multicare. E. Aygören-Pürsün has received grants from CSL Behring and Takeda and consulting fees from CSL Behring, Biocryst, KalVista and Pharvaris. He has received speaker fees from CSL Behring, Biocryst, Centogene, Pharming and Takeda and has received fees as an advisor for Astria, Biocryst, BioMarin Europe, Centogene, CSL Behring, Intellia, KalVista, Pharming, Pharvaris and Takeda. N. Bara has received grants from Takeda and has received payment for lectures/presentations from Takeda, Pharming and CSL Behring. She has participated in advisory boards for Takeda, Pharming, KalVista and Biocryst and has participated in a committee or advocacy group for the Romanian Registry for the HAE Foundation, the Roman Society of Allergy and Clinical Immunology and is head of the Romanian Expert Committee for Hereditary Angioedema. M. Ben-Shoshan is or recently was a speaker and/or advisor for Sanofi and Novartis. J. Bernstein has received grants from Takeda/Shire, CSL Behring, Pharming, Biocryst, Biomarin, Ionis Pharmaceuticals, KalVista, Sanofi, Regeneron, Astra Zeneca, Amgen, Novartis, Genentech, Celldex, Jasper, Escient, Allakos, Blueprint Medicine, Cogent, Telios, Astria and Teva. He has received consulting fees from Pharvaris and is the president of AAAAI. S. Betschel has received payment for lectures/presentations from Biocryst, CSL Behring, KalVista and Takeda and has received travel support from Biocryst, CSL Behring, KalVista and Takeda. He has participated in advisory boards for Ionis Pharmaceuticals, Pharvaris, Takeda, CSL Behring, Novartis, Astria and Biocryst. He is the voluntary chair of the Canadian Hereditary Angioedema Network. L. Bouillet has received consulting fees and has received payment or honoraria from CSL Behring, Takeda, Biocryst, Pharvaris, Novartis and GlaxoSmithKline. He has attended meetings for CSL Behring, Takeda, Biocryst, Novartis and GlaxoSmithKline and has participated in advisory boards for CSL Behring, Takeda, Biocryst, Pharvaris, Intellia and KalVista. He is in a leadership position for the SNFMI (French Internal Medicine Society). T. Caballero has no conflicts of interest in relation to this work. Outside it, she has participated in advisory boards for Astria, Biocryst, CSL Behring, KalVista, Novartis, Pharming, Pharvaris and Takeda. She is a member of speaker bureaus for Biocryst, CSL Behring, Novartis, Pharming and Takeda and has received grants from CSL Behring and Takeda. She has received funding to attend conferences/educational events from Biocryst, CSL Behring, Novartis, Pharming and Takeda and is/has been a clinical trial/registry investigator for Biocryst, CSL Behring, Ionis Pharmaceuticals, KalVista, Novartis, Pharming and Takeda. She is a researcher from the IdiPAZ programme for promoting research activities. M. Cancian has received personal fees from Biocryst, CSL Behring, KalVista and Takeda. A. J. Castaldo has no conflicts of interest. S. Cimbollek was a speaker and/or advisor for and/or received research funding from Takeda, Novartis, Pharming, CSL Behring, Biocryst, GlaxoSmithKline, Sanofi/Regeneron and Astra Zeneca. D. M. Cohn has received speaking fees from CSL Behring, Ionis Pharmaceuticals, Pharvaris and Takeda and consultancy fees from Astria, Biocryst, CSL Behring, Ionis Pharmaceuticals, KalVista, Pharming, Pharvaris and Takeda. He has received research support from Ionis Pharmaceuticals, KalVista, Pharvaris and Takeda. T. Craig has served as a speaker and researcher for Biomarin, CSL Behring, Intellia and Takeda and has been a researcher for Astria, Ionis Pharmaceuticals, KalVista and Pharvaris. He has been a speaker for Grifols and a consultant for Astria, Biocryst, Biomarin, CSL Behring, Intellia and Spark. He is the director of ACARE International Hereditary Angioedema Center and a member of the Medical Advisory Board for the HAE-A. D. Fomina has no conflicts in relation to this work. A. Gelincik is or recently was a speaker and/or advisor for Takeda and Pharvaris and has received research funding from Ionis Pharmaceuticals, Takeda and Pharvaris. V. Grivcheva-Panovska has received travel support from Pharming and Takeda. A. Jindal has no conflicts of interest in relation to this work. C. Katelaris has received institutional funding as a Principal Investigator on clinical trials for CSL Behring, KVD Pharma, Intellia and Biocryst and has received payments for presentations and advisory board participation from CSL Behring, Takeda, Phavaris, KVD Pharma, GlaxoSmithKline, Menarini, Novartis and Sanofi. A. Kessel has received consulting fees from Biocryst, KalVista and Takeda and has received payment for lectures/presentations from Takeda. He has received travel support from Takeda and has participated in advisory boards for KalVista and Takeda. He has received equipment or services from Takeda. T. Kinaciyan is or recently was a speaker and/or advisor for and/or has received research funding from Biocryst, CSL Behring, KalVista Pharmaceuticals, Pharming, Pharvaris, Sanofi and Takeda. H. Longhurst is or recently was a speaker and/or advisor for and/or has received research funding from CSL Behring, Intellia, KalVista, Pharming and Takeda I. Martinez-Saguer is recently or was a speaker and/or advisor for and/or has received research funding from Biocryst, CSL Behring, KalVista, Pharming, Pharvaris, Octapharma and Takeda. M. Riedl has received research grants from Biocryst, Biomarin, CSL Behring, Ionis Pharmaceuticals, KalVista, Pharvaris and Takeda and has served as a consultant for Astria, Biocryst, Biomarin, Celldex, CSL Behring, Cycle Pharma, Grifols, Intellia, KalVista, Pfizer, Pharming, Pharvaris, Sanofi-Regeneron and Takeda. C. Schöffl has received payment for lectures/presentations from Biocryst, CSL Behring, KalVista and Takeda and has received travel support from Biocryst, CSL Behring and Takeda. He has participated in advisory boards for Biocryst, CSL Behring, KalVista and Takeda and is a board member of the Austrian HAE member organisation. P. Staubach has no conflicts in relation to this work. Outside it, she has received grants from Novartis and Sanofi and has received consulting fees from CSL Behring, Octapharma, Novartis, Biocryst, Takeda, Sanofi/Regeneron and Genzyme. She is a member of the Society of Dermopharmazie. A. Zanichelli has received honoraria as a speaker/advisor from Biocryst, CSL Behring, KalVista, Pharming, Pharvaris and Takeda. Y-X. Zhi has no conflicts of interest in relation to this work. H. B. Boysen has no conflicts of interest in relation to this work. Jie Shen Fok has received payments for lectures/presentations from Viatris, Novartis, CSL Behring and Takeda and has received travel support from Viatris, CSL Behring and Takeda. Philip Li has no conflicts in relation to this work. R. Hakl has no conflicts of interest in relation to this work. Outside it, he has received consultancy/speaker honoraria from CSL Behring, Shire and Takeda and has served as a principal investigator for clinical trials sponsored by Biocryst, Pharvaris, Pharming, CSL Behring and KalVista. M. Hide is or recently was a speaker and/or advisor for CSL Behring, Eisai, Kaken, KalVista, Kyorin, Kyowa-Kirin, Meiji, Mitsubishi Tanabe Pharma, Nippon Zoki, Novartis, Pharvaris, Sanofi/Regeneron, Taiho, Takeda, Teikoku and Torii. J. Peter is or recently was a speaker and/or advisor for and/or has received research funding from Abbivie, AstraZeneca, Astria, Biocryst, CSL Behring, GlaxoSmithKline, Glenmark, KalVista, Novartis, Pharvaris, Sanofi/Regeneron, Takeda and Johnson & Johnson. M. Maurer is or recently was a speaker and/or advisor for and/or has received research funding from Allakos, Alvotech, Amgen, Aquestive, Aralez, AstraZeneca, Astria, Bayer, Biocryst, Blueprint, Celldex, Celltrion, Centogene, CSL Behring, Evommune, GlaxoSmithKline, Ipsen, KalVista, Kyowa Kirin, Leo Pharma, Lilly, Menarini, Mitsubishi Tanabe Pharma, Moxie, Noucor, Novartis, Orion Biotechnology, Pharvaris, Resonance Medicine, Sanofi/Regeneron, Septerna, Takeda, Teva, Third HarmonicBio, Valenza Bio, Yuhan Corporation and Zurabio.</p><p>The CARE study received initial approval in August 2023 from the Ethics Committee of Charité—Universitätsmedizin Berlin (reference no.: EA2/145/23). All other participating institutions must obtain approval from their respective ethics committees as required by national laws before being included in the registry.</p>\",\"PeriodicalId\":10207,\"journal\":{\"name\":\"Clinical and Experimental Allergy\",\"volume\":\"54 9\",\"pages\":\"712-716\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-06-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14527\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cea.14527\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14527","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
The Chronic Angioedema Registry (CARE): Rationale, Methods and Implementation
Angioedema (AE) is a paroxysmal, localised and self-limiting swelling of the subcutaneous and/or submucosal tissue, because of a temporary increase in vascular permeability. Recurrent AE is a heterogeneous disease, which is categorised into different types [1]. Clinical and sociodemographic core factors in AE remain insufficiently investigated. A need exists for a large, comprehensive worldwide registry for all types of recurrent AE, applying modern methodologies and parameters from recent scientific knowledge.
Chronic Angioedema Registry (CARE) is an international, prospective, multicentre, observational (noninterventional), open-ended disease registry initiated in 2023 by the global network of Angioedema Centers of Reference and Excellence (ACARE) and the Urticaria Network e.V. (UNEV), which aims to enhance the understanding of recurrent AE of all aetiologies in worldwide clinical settings.
All physicians treating patients with AE, irrespective of location, medical specialty or setting, are invited to participate in CARE. The requirements for participation and the ‘Project Plan’ and ‘CARE Charter’ can be found on the CARE website (https://chronic-angioedema-registry.com). Participation in CARE incurs no costs, no financial compensation or support is provided, and no charges will be billed to health insurers. Data submission is voluntary and solely at the physician and patient's discretion.
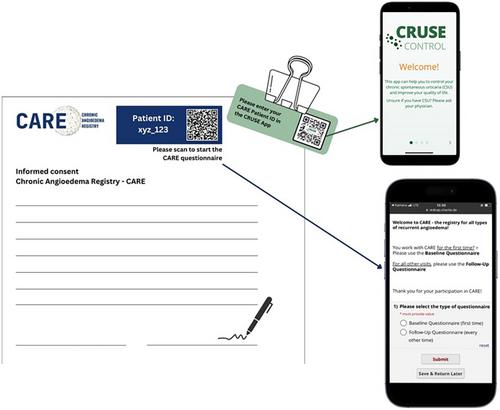
The CARE questionnaires, developed by the CARE International Steering Committee (ISC), consist of basic multiple-choice or short-answer questions. Questions and variables are programmed in REDCap (Nashville, Tennessee), a secure, web-based software platform designed to support data capture for research studies (https://www.project-redcap.org; downloaded on 5 July 2023). After giving their written informed consent, participating patients receive a QR code linked to their participant identification (ID) number, allowing them to access the patient questionnaire via a smart device; the treating physician gets the patient's ID and completes the physician questionnaire (Figure 1).
CARE data will be collected during routine patient consultation visits and examinations for AE treatment. CARE will continue to follow patients as long as the physician and patient are considered appropriate. Data will be transferred at regular periods from REDCap into an electronic case report form programme to process and monitor the data. Outlier and diagnostic plots are used to check for plausibility, consistency and integrity.
The registry database is owned, hosted and administered by UNEV. Participating physicians are responsible for retaining all source data, and the staff of the treating physician must monitor and manage the patient's data. If patients withdraw their consent, their data will not be further included. A patient's previous data will be deleted from the registry upon a patient's request.
Patient baseline and follow-up questionnaires can be completed within 20 and 15 min, respectively, and are developed in different languages. Both questionnaires contain pictures and descriptions of AE and wheals to ensure patients comprehend the distinctions. Baseline questionnaires collect data on patient's demographics, disease duration, disease course, frequency, underlying causes, comorbidities, triggering factors, treatments, disease activity, disease control, quality of life impairment and direct healthcare costs. Follow-up questionnaires gather data about changes in the patient's signs and symptoms, disease control, quality of life, treatments and healthcare usage. No time point for follow-up data collection is specified, but this should occur between 3 months and 1 year. In both patient questionnaires, the Angioedema Control Test and the Angioedema Quality of Life Questionnaire are used to assess disease control and disease-related quality of life, respectively [2, 3]. In the physician baseline and follow-up questionnaires, the treating physician reports the type of AE.
Participating physicians may analyse and publish CARE data. They can obtain a spreadsheet of raw data by submitting a ‘Request for Analysis’ to UNEV. The CARE ISC will help manage publications, and the proposing physician will lead the group of coauthors. Physicians retain the right to independently analyse, present and publish their data without seeking approval from the CARE ISC, but their publications must acknowledge the CARE project's contributions.
CARE is subjected to the typical limitations that apply to observational studies and specific constraints associated with registries. Many participating physicians/sites have specialised AE expertise, leading to a likelihood that enrolled patients have more complex conditions and severe forms. Consequently, the outcomes derived from CARE may not broadly apply to less severe cases of AE typically seen in primary care or community settings. In addition, participating physicians are not obligated to continuously register all AE patients, leading to an unintended selection bias. Furthermore, the findings may not always be generalisable to patients globally or those from diverse ethnic backgrounds.
Although a few international and national registries on AE have been previously initiated, they had relatively small patient numbers, assessed a limited number of parameters and exclusively focussed on either hereditary angioedema or chronic urticaria [4-6]. Because of its large patient size, CARE has the potential to detect and assess even rare forms of AE and to elicit treatment responses. In future, CARE will benefit from joint analyses with other registries, such as the Chronic Urticaria Registry, as further assessments of the overlap between different AE types could better understand disease phenotypes, link pathogenic drivers and guide patient care [5, 7, 8]. Additionally, once CARE data start being recorded, it could be linked to currently used patient apps such as CRUSE, a patient app used to monitor and control chronic urticaria, or to patient biobank blood samples [9].
In conclusion, CARE could become the most modern, comprehensive research project on recurrent AE of all aetiologies. Collecting real-life data in CARE will equip physicians and researchers with better information on managing, monitoring and improving patient care in AE.
T. Buttgereit, F. Aulenbacher, A. Gutsche, M. Maurer, M. Magerl and K. Weller designed the study with input from all authors. T. Buttgereit and M. Maurer prepared the main manuscript text. All authors contributed to writing or reviewing the manuscript and final approval.
T. Buttgereit is or recently was a speaker and/or advisor for Aquestive, AstraZeneca, Biocryst, CSL-Behring, GlaxoSmithKline, Hexal, KalVista, Medac, Novartis, Pharming, Pharvaris, Roche, Sanofi, Swixx BioPharma and Takeda. P. Kolkhir has been a speaker for Novartis, ValenzaBio and Roche. A. Gutsche has no conflicts of interest in relation to this work. F. Aulenbacher has no conflicts of interest in relation to this work. K. Weller has no conflicts of interest in relation to this work. Outside it, he is or recently was a speaker and/or advisor for and/or has received research funding from Biocryst, CSL-Behring, Moxie, Novartis, Sanofi and Takeda. C. Vera Ayala has no conflicts of interest in relation to this work. M. Magerl is or recently was a speaker and/or advisor for and/or has received research funding from Biocryst, Pharming, Takeda, CSL Behring, Ionis Pharmaceuticals, KalVista and Pharvaris. H. Farkas has no conflicts of interest in relation to this work. Outside it, she has received research grants from CSL Behring, Takeda and Pharming. She was a speaker and/or advisor for CSL Behring, Takeda, Pharming KalVista, ONO Pharmaceutical, Pharvaris, Astria, Intellia and Biocryst. A. S. Grumach has no conflicts of interest in relation to this work. She has received a grant from the Brazilian National Council of Research (CNPq) and Takeda and is or recently was a speaker and/or advisor for Takeda, CSL-Behring, Pharvaris, KalVista, Exeltis, Pint-Pharma, Biomarin, Binding site and Multicare. E. Aygören-Pürsün has received grants from CSL Behring and Takeda and consulting fees from CSL Behring, Biocryst, KalVista and Pharvaris. He has received speaker fees from CSL Behring, Biocryst, Centogene, Pharming and Takeda and has received fees as an advisor for Astria, Biocryst, BioMarin Europe, Centogene, CSL Behring, Intellia, KalVista, Pharming, Pharvaris and Takeda. N. Bara has received grants from Takeda and has received payment for lectures/presentations from Takeda, Pharming and CSL Behring. She has participated in advisory boards for Takeda, Pharming, KalVista and Biocryst and has participated in a committee or advocacy group for the Romanian Registry for the HAE Foundation, the Roman Society of Allergy and Clinical Immunology and is head of the Romanian Expert Committee for Hereditary Angioedema. M. Ben-Shoshan is or recently was a speaker and/or advisor for Sanofi and Novartis. J. Bernstein has received grants from Takeda/Shire, CSL Behring, Pharming, Biocryst, Biomarin, Ionis Pharmaceuticals, KalVista, Sanofi, Regeneron, Astra Zeneca, Amgen, Novartis, Genentech, Celldex, Jasper, Escient, Allakos, Blueprint Medicine, Cogent, Telios, Astria and Teva. He has received consulting fees from Pharvaris and is the president of AAAAI. S. Betschel has received payment for lectures/presentations from Biocryst, CSL Behring, KalVista and Takeda and has received travel support from Biocryst, CSL Behring, KalVista and Takeda. He has participated in advisory boards for Ionis Pharmaceuticals, Pharvaris, Takeda, CSL Behring, Novartis, Astria and Biocryst. He is the voluntary chair of the Canadian Hereditary Angioedema Network. L. Bouillet has received consulting fees and has received payment or honoraria from CSL Behring, Takeda, Biocryst, Pharvaris, Novartis and GlaxoSmithKline. He has attended meetings for CSL Behring, Takeda, Biocryst, Novartis and GlaxoSmithKline and has participated in advisory boards for CSL Behring, Takeda, Biocryst, Pharvaris, Intellia and KalVista. He is in a leadership position for the SNFMI (French Internal Medicine Society). T. Caballero has no conflicts of interest in relation to this work. Outside it, she has participated in advisory boards for Astria, Biocryst, CSL Behring, KalVista, Novartis, Pharming, Pharvaris and Takeda. She is a member of speaker bureaus for Biocryst, CSL Behring, Novartis, Pharming and Takeda and has received grants from CSL Behring and Takeda. She has received funding to attend conferences/educational events from Biocryst, CSL Behring, Novartis, Pharming and Takeda and is/has been a clinical trial/registry investigator for Biocryst, CSL Behring, Ionis Pharmaceuticals, KalVista, Novartis, Pharming and Takeda. She is a researcher from the IdiPAZ programme for promoting research activities. M. Cancian has received personal fees from Biocryst, CSL Behring, KalVista and Takeda. A. J. Castaldo has no conflicts of interest. S. Cimbollek was a speaker and/or advisor for and/or received research funding from Takeda, Novartis, Pharming, CSL Behring, Biocryst, GlaxoSmithKline, Sanofi/Regeneron and Astra Zeneca. D. M. Cohn has received speaking fees from CSL Behring, Ionis Pharmaceuticals, Pharvaris and Takeda and consultancy fees from Astria, Biocryst, CSL Behring, Ionis Pharmaceuticals, KalVista, Pharming, Pharvaris and Takeda. He has received research support from Ionis Pharmaceuticals, KalVista, Pharvaris and Takeda. T. Craig has served as a speaker and researcher for Biomarin, CSL Behring, Intellia and Takeda and has been a researcher for Astria, Ionis Pharmaceuticals, KalVista and Pharvaris. He has been a speaker for Grifols and a consultant for Astria, Biocryst, Biomarin, CSL Behring, Intellia and Spark. He is the director of ACARE International Hereditary Angioedema Center and a member of the Medical Advisory Board for the HAE-A. D. Fomina has no conflicts in relation to this work. A. Gelincik is or recently was a speaker and/or advisor for Takeda and Pharvaris and has received research funding from Ionis Pharmaceuticals, Takeda and Pharvaris. V. Grivcheva-Panovska has received travel support from Pharming and Takeda. A. Jindal has no conflicts of interest in relation to this work. C. Katelaris has received institutional funding as a Principal Investigator on clinical trials for CSL Behring, KVD Pharma, Intellia and Biocryst and has received payments for presentations and advisory board participation from CSL Behring, Takeda, Phavaris, KVD Pharma, GlaxoSmithKline, Menarini, Novartis and Sanofi. A. Kessel has received consulting fees from Biocryst, KalVista and Takeda and has received payment for lectures/presentations from Takeda. He has received travel support from Takeda and has participated in advisory boards for KalVista and Takeda. He has received equipment or services from Takeda. T. Kinaciyan is or recently was a speaker and/or advisor for and/or has received research funding from Biocryst, CSL Behring, KalVista Pharmaceuticals, Pharming, Pharvaris, Sanofi and Takeda. H. Longhurst is or recently was a speaker and/or advisor for and/or has received research funding from CSL Behring, Intellia, KalVista, Pharming and Takeda I. Martinez-Saguer is recently or was a speaker and/or advisor for and/or has received research funding from Biocryst, CSL Behring, KalVista, Pharming, Pharvaris, Octapharma and Takeda. M. Riedl has received research grants from Biocryst, Biomarin, CSL Behring, Ionis Pharmaceuticals, KalVista, Pharvaris and Takeda and has served as a consultant for Astria, Biocryst, Biomarin, Celldex, CSL Behring, Cycle Pharma, Grifols, Intellia, KalVista, Pfizer, Pharming, Pharvaris, Sanofi-Regeneron and Takeda. C. Schöffl has received payment for lectures/presentations from Biocryst, CSL Behring, KalVista and Takeda and has received travel support from Biocryst, CSL Behring and Takeda. He has participated in advisory boards for Biocryst, CSL Behring, KalVista and Takeda and is a board member of the Austrian HAE member organisation. P. Staubach has no conflicts in relation to this work. Outside it, she has received grants from Novartis and Sanofi and has received consulting fees from CSL Behring, Octapharma, Novartis, Biocryst, Takeda, Sanofi/Regeneron and Genzyme. She is a member of the Society of Dermopharmazie. A. Zanichelli has received honoraria as a speaker/advisor from Biocryst, CSL Behring, KalVista, Pharming, Pharvaris and Takeda. Y-X. Zhi has no conflicts of interest in relation to this work. H. B. Boysen has no conflicts of interest in relation to this work. Jie Shen Fok has received payments for lectures/presentations from Viatris, Novartis, CSL Behring and Takeda and has received travel support from Viatris, CSL Behring and Takeda. Philip Li has no conflicts in relation to this work. R. Hakl has no conflicts of interest in relation to this work. Outside it, he has received consultancy/speaker honoraria from CSL Behring, Shire and Takeda and has served as a principal investigator for clinical trials sponsored by Biocryst, Pharvaris, Pharming, CSL Behring and KalVista. M. Hide is or recently was a speaker and/or advisor for CSL Behring, Eisai, Kaken, KalVista, Kyorin, Kyowa-Kirin, Meiji, Mitsubishi Tanabe Pharma, Nippon Zoki, Novartis, Pharvaris, Sanofi/Regeneron, Taiho, Takeda, Teikoku and Torii. J. Peter is or recently was a speaker and/or advisor for and/or has received research funding from Abbivie, AstraZeneca, Astria, Biocryst, CSL Behring, GlaxoSmithKline, Glenmark, KalVista, Novartis, Pharvaris, Sanofi/Regeneron, Takeda and Johnson & Johnson. M. Maurer is or recently was a speaker and/or advisor for and/or has received research funding from Allakos, Alvotech, Amgen, Aquestive, Aralez, AstraZeneca, Astria, Bayer, Biocryst, Blueprint, Celldex, Celltrion, Centogene, CSL Behring, Evommune, GlaxoSmithKline, Ipsen, KalVista, Kyowa Kirin, Leo Pharma, Lilly, Menarini, Mitsubishi Tanabe Pharma, Moxie, Noucor, Novartis, Orion Biotechnology, Pharvaris, Resonance Medicine, Sanofi/Regeneron, Septerna, Takeda, Teva, Third HarmonicBio, Valenza Bio, Yuhan Corporation and Zurabio.
The CARE study received initial approval in August 2023 from the Ethics Committee of Charité—Universitätsmedizin Berlin (reference no.: EA2/145/23). All other participating institutions must obtain approval from their respective ethics committees as required by national laws before being included in the registry.
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
