{"title":"模拟脱屑性炎症性外阴阴道炎的外阴阴道扁平苔藓:病例系列。","authors":"Marlene Wijaya BMed, MD, MPhil, Rebecca Bronwyn Saunderson BMedSci (hon1), MBBS (hon), MPhil (Cantab), FACD, Gayle Fischer MBBS (hon1), MD, FACD","doi":"10.1111/ajd.14344","DOIUrl":null,"url":null,"abstract":"<p>Vulvovaginal lichen planus (VLP) is a chronic inflammatory dermatosis of the vulva with or without vaginal involvement. Its diagnosis can be challenging due to variations in morphology and histopathological findings. In 1988, Edwards and Friedrich reported a case series of VLP patients whose clinical presentation mimicked desquamative inflammatory vulvovaginitis (DIV).<span><sup>1</sup></span> DIV is an uncommon non-infective vulvovaginitis, characterised by pain, dyspareunia, pruritus and white or green non-offensive discharge. However, unlike VLP is not a scarring condition.<span><sup>2</sup></span> Herein we present a case series of women who were initially diagnosed with DIV but did not respond to treatment with topical clindamycin which is usually highly effective (Table 1). When their diagnosis was revised, they improved following treatment appropriate for VLP.</p><p>To our knowledge, this is the only other case series since 1988 to report patients with DIV-like VLP. DIV and VLP can pose significant diagnostic challenges as both have a wide range of clinical manifestations and histopathological findings, which often overlap. On histology, lichenoid infiltrate can be found in either condition, and the observed changes are often reported as ‘non-specific’. Additionally, the two conditions have a predilection for peri-/post-menopausal women.<span><sup>3, 4</sup></span></p><p>Desquamative inflammatory vulvovaginitis is typically characterised by vulval pain, dyspareunia and purulent white or green non-offensive discharge.<span><sup>5, 6</sup></span> Erythema and petechiae or punctate erosions are usually observed on examination.<span><sup>2, 3</sup></span> Meanwhile, in VLP, purulent discharge is not normally observed. DIV does not result in scarring, whereas VLP typically presents with glazed erythema, erosions and hyperkeratosis and frequently, if untreated causes scarring, loss of vulval structure and stenosis of the vagina.<span><sup>7</sup></span> There can also be associated oral mucosal involvement (oral lichen planus) which is not observed in DIV. In our case series, petechiae were consistently observed in all patients. This suggests that although petechiae are not common findings in VLP,<span><sup>8</sup></span> these may re-present a small sub-type of VLP mimicking DIV. Additionally, as in case 3, oral mucosal involvement may provide an additional clue pointing to a diagnosis of VLP.</p><p>Treatment resistance should also prompt clinicians to consider an alternative diagnosis, as DIV usually responds promptly to topical antibiotic treatments, particularly 2% clindamycin. A study by Bradford et al. compared 101 cases of DIV to 75 cases of VLP.<span><sup>2</sup></span> The majority of DIV patients (94%) were responsive to 4–6 weeks of intravaginal clindamycin 2%, with 35% requiring maintenance therapy. In another study by Sobel et al. of 130 DIV patients over a 12-year period, 86% of the patients reported significant symptom improvement within 3 weeks of being commenced on clindamycin 2% or hydrocortisone 10% cream.</p><p>Historical triggers have been reported as potential differentiators between DIV and VLP. In the study by Bradford et al., more than half of DIV patients (56%) reported historical triggers, compared to only 15% in the VLP group (<i>p</i> < 0.0001).<span><sup>2</sup></span> Some of the documented triggers included diarrhoea, prolonged antibiotic use and acute genital infection. In the presented case series, two patients had suspected chronic vulvovaginal candidiasis (CVVC). One patient had a drug reaction with eosinophilia and systemic symptoms (DRESS) due to lamotrigine prior to the disease onset.</p><p>It would also appear that DIV like VLP is a challenge to treat. Only one of our patients was able to achieve control with topical corticosteroids with all others requiring systemic treatments.</p><p>In summary, VLP can present with signs and symptoms mimicking DIV. In patients who have been diagnosed with DIV and demonstrate treatment resistance, an alternative diagnosis of VLP should be considered. The involvement of other body sites, such as oral mucosa, can also help in making the diagnosis of VLP. This subgroup of VLP appears to require systemic treatment in most cases.</p><p>None reported.</p><p>Ethics approval has been obtained from the Ramsay Health Care Human Research Ethics Committee.</p><p>All patients have consented to the inclusion of their cases in this report for journal publication. Consent has been obtained from patients, whose photos are included in this report.</p>","PeriodicalId":8638,"journal":{"name":"Australasian Journal of Dermatology","volume":"65 7","pages":"e203-e207"},"PeriodicalIF":1.8000,"publicationDate":"2024-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ajd.14344","citationCount":"0","resultStr":"{\"title\":\"Vulvovaginal lichen planus mimicking desquamative inflammatory vulvovaginitis: A case series\",\"authors\":\"Marlene Wijaya BMed, MD, MPhil, Rebecca Bronwyn Saunderson BMedSci (hon1), MBBS (hon), MPhil (Cantab), FACD, Gayle Fischer MBBS (hon1), MD, FACD\",\"doi\":\"10.1111/ajd.14344\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Vulvovaginal lichen planus (VLP) is a chronic inflammatory dermatosis of the vulva with or without vaginal involvement. Its diagnosis can be challenging due to variations in morphology and histopathological findings. In 1988, Edwards and Friedrich reported a case series of VLP patients whose clinical presentation mimicked desquamative inflammatory vulvovaginitis (DIV).<span><sup>1</sup></span> DIV is an uncommon non-infective vulvovaginitis, characterised by pain, dyspareunia, pruritus and white or green non-offensive discharge. However, unlike VLP is not a scarring condition.<span><sup>2</sup></span> Herein we present a case series of women who were initially diagnosed with DIV but did not respond to treatment with topical clindamycin which is usually highly effective (Table 1). When their diagnosis was revised, they improved following treatment appropriate for VLP.</p><p>To our knowledge, this is the only other case series since 1988 to report patients with DIV-like VLP. DIV and VLP can pose significant diagnostic challenges as both have a wide range of clinical manifestations and histopathological findings, which often overlap. On histology, lichenoid infiltrate can be found in either condition, and the observed changes are often reported as ‘non-specific’. Additionally, the two conditions have a predilection for peri-/post-menopausal women.<span><sup>3, 4</sup></span></p><p>Desquamative inflammatory vulvovaginitis is typically characterised by vulval pain, dyspareunia and purulent white or green non-offensive discharge.<span><sup>5, 6</sup></span> Erythema and petechiae or punctate erosions are usually observed on examination.<span><sup>2, 3</sup></span> Meanwhile, in VLP, purulent discharge is not normally observed. DIV does not result in scarring, whereas VLP typically presents with glazed erythema, erosions and hyperkeratosis and frequently, if untreated causes scarring, loss of vulval structure and stenosis of the vagina.<span><sup>7</sup></span> There can also be associated oral mucosal involvement (oral lichen planus) which is not observed in DIV. In our case series, petechiae were consistently observed in all patients. This suggests that although petechiae are not common findings in VLP,<span><sup>8</sup></span> these may re-present a small sub-type of VLP mimicking DIV. Additionally, as in case 3, oral mucosal involvement may provide an additional clue pointing to a diagnosis of VLP.</p><p>Treatment resistance should also prompt clinicians to consider an alternative diagnosis, as DIV usually responds promptly to topical antibiotic treatments, particularly 2% clindamycin. A study by Bradford et al. compared 101 cases of DIV to 75 cases of VLP.<span><sup>2</sup></span> The majority of DIV patients (94%) were responsive to 4–6 weeks of intravaginal clindamycin 2%, with 35% requiring maintenance therapy. In another study by Sobel et al. of 130 DIV patients over a 12-year period, 86% of the patients reported significant symptom improvement within 3 weeks of being commenced on clindamycin 2% or hydrocortisone 10% cream.</p><p>Historical triggers have been reported as potential differentiators between DIV and VLP. In the study by Bradford et al., more than half of DIV patients (56%) reported historical triggers, compared to only 15% in the VLP group (<i>p</i> < 0.0001).<span><sup>2</sup></span> Some of the documented triggers included diarrhoea, prolonged antibiotic use and acute genital infection. In the presented case series, two patients had suspected chronic vulvovaginal candidiasis (CVVC). One patient had a drug reaction with eosinophilia and systemic symptoms (DRESS) due to lamotrigine prior to the disease onset.</p><p>It would also appear that DIV like VLP is a challenge to treat. Only one of our patients was able to achieve control with topical corticosteroids with all others requiring systemic treatments.</p><p>In summary, VLP can present with signs and symptoms mimicking DIV. In patients who have been diagnosed with DIV and demonstrate treatment resistance, an alternative diagnosis of VLP should be considered. The involvement of other body sites, such as oral mucosa, can also help in making the diagnosis of VLP. This subgroup of VLP appears to require systemic treatment in most cases.</p><p>None reported.</p><p>Ethics approval has been obtained from the Ramsay Health Care Human Research Ethics Committee.</p><p>All patients have consented to the inclusion of their cases in this report for journal publication. Consent has been obtained from patients, whose photos are included in this report.</p>\",\"PeriodicalId\":8638,\"journal\":{\"name\":\"Australasian Journal of Dermatology\",\"volume\":\"65 7\",\"pages\":\"e203-e207\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-07-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ajd.14344\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Australasian Journal of Dermatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ajd.14344\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Australasian Journal of Dermatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ajd.14344","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
外阴阴道扁平苔藓(VLP)是一种慢性外阴炎症性皮肤病,可累及或不累及阴道。由于形态学和组织病理学结果的差异,其诊断可能具有挑战性。1 DIV是一种不常见的非感染性外阴阴道炎,以疼痛、排便困难、瘙痒和白色或绿色非致病性分泌物为特征。1 DIV 是一种不常见的非感染性外阴阴道炎,其特征是疼痛、排便困难、瘙痒和白色或绿色非排泄性分泌物,但与 VLP 不同的是,它不是一种瘢痕性疾病。2 在此,我们介绍了一组病例,这些妇女最初被诊断为 DIV,但对通常非常有效的外用克林霉素治疗无效(表 1)。据我们所知,这是自1988年以来报告的唯一一个类似DIV的VLP患者病例系列。DIV和VLP会给诊断带来巨大挑战,因为这两种疾病的临床表现和组织病理学检查结果多种多样,而且往往相互重叠。在组织学上,这两种疾病都会出现苔藓样浸润,而观察到的变化往往被报告为 "非特异性"。5、6 检查时通常会观察到红斑、瘀点或点状糜烂。2、3 同时,在 VLP 中通常观察不到脓性分泌物。DIV 不会导致瘢痕形成,而 VLP 通常表现为釉面红斑、糜烂和角化过度,如果不及时治疗,常常会导致瘢痕形成、外阴结构缺失和阴道狭窄。在我们的病例系列中,所有患者均可观察到瘀斑。这表明,虽然瘀斑在 VLP 中并不常见,8 但这些瘀斑可能是模仿 DIV 的 VLP 的一个小亚型。此外,与病例 3 一样,口腔粘膜受累也可能为 VLP 诊断提供额外线索。耐药性也应促使临床医生考虑其他诊断,因为 DIV 通常对局部抗生素治疗反应迅速,尤其是 2% 的克林霉素。Bradford 等人的一项研究比较了 101 例 DIV 和 75 例 VLP。2 大多数 DIV 患者(94%)对阴道内使用 4-6 周 2% 的克林霉素有反应,其中 35% 需要维持治疗。在 Sobel 等人对 130 名 DIV 患者进行的另一项为期 12 年的研究中,86% 的患者在开始使用 2% 的克林霉素或 10%的氢化可的松乳膏 3 周内症状明显改善。在 Bradford 等人的研究中,半数以上的 DIV 患者(56%)报告了历史诱因,而 VLP 组仅为 15%(p < 0.0001)2。在本系列病例中,有两名患者疑似患有慢性外阴阴道念珠菌病(CVVC)。一名患者在发病前曾因服用拉莫三嗪而出现伴有嗜酸性粒细胞增多和全身症状的药物反应(DRESS)。我们的患者中只有一人能够通过外用皮质类固醇得到控制,其他人都需要系统治疗。对于已确诊为 DIV 并表现出抗药性的患者,应考虑 VLP 的替代诊断。其他身体部位(如口腔粘膜)受累也有助于 VLP 的诊断。所有患者均同意将其病例纳入本报告并在期刊上发表。本报告中包含的患者照片已征得患者同意。
Vulvovaginal lichen planus mimicking desquamative inflammatory vulvovaginitis: A case series
Vulvovaginal lichen planus (VLP) is a chronic inflammatory dermatosis of the vulva with or without vaginal involvement. Its diagnosis can be challenging due to variations in morphology and histopathological findings. In 1988, Edwards and Friedrich reported a case series of VLP patients whose clinical presentation mimicked desquamative inflammatory vulvovaginitis (DIV).1 DIV is an uncommon non-infective vulvovaginitis, characterised by pain, dyspareunia, pruritus and white or green non-offensive discharge. However, unlike VLP is not a scarring condition.2 Herein we present a case series of women who were initially diagnosed with DIV but did not respond to treatment with topical clindamycin which is usually highly effective (Table 1). When their diagnosis was revised, they improved following treatment appropriate for VLP.
To our knowledge, this is the only other case series since 1988 to report patients with DIV-like VLP. DIV and VLP can pose significant diagnostic challenges as both have a wide range of clinical manifestations and histopathological findings, which often overlap. On histology, lichenoid infiltrate can be found in either condition, and the observed changes are often reported as ‘non-specific’. Additionally, the two conditions have a predilection for peri-/post-menopausal women.3, 4
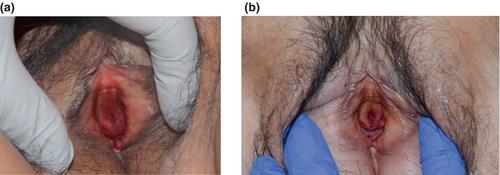
Desquamative inflammatory vulvovaginitis is typically characterised by vulval pain, dyspareunia and purulent white or green non-offensive discharge.5, 6 Erythema and petechiae or punctate erosions are usually observed on examination.2, 3 Meanwhile, in VLP, purulent discharge is not normally observed. DIV does not result in scarring, whereas VLP typically presents with glazed erythema, erosions and hyperkeratosis and frequently, if untreated causes scarring, loss of vulval structure and stenosis of the vagina.7 There can also be associated oral mucosal involvement (oral lichen planus) which is not observed in DIV. In our case series, petechiae were consistently observed in all patients. This suggests that although petechiae are not common findings in VLP,8 these may re-present a small sub-type of VLP mimicking DIV. Additionally, as in case 3, oral mucosal involvement may provide an additional clue pointing to a diagnosis of VLP.
Treatment resistance should also prompt clinicians to consider an alternative diagnosis, as DIV usually responds promptly to topical antibiotic treatments, particularly 2% clindamycin. A study by Bradford et al. compared 101 cases of DIV to 75 cases of VLP.2 The majority of DIV patients (94%) were responsive to 4–6 weeks of intravaginal clindamycin 2%, with 35% requiring maintenance therapy. In another study by Sobel et al. of 130 DIV patients over a 12-year period, 86% of the patients reported significant symptom improvement within 3 weeks of being commenced on clindamycin 2% or hydrocortisone 10% cream.
Historical triggers have been reported as potential differentiators between DIV and VLP. In the study by Bradford et al., more than half of DIV patients (56%) reported historical triggers, compared to only 15% in the VLP group (p < 0.0001).2 Some of the documented triggers included diarrhoea, prolonged antibiotic use and acute genital infection. In the presented case series, two patients had suspected chronic vulvovaginal candidiasis (CVVC). One patient had a drug reaction with eosinophilia and systemic symptoms (DRESS) due to lamotrigine prior to the disease onset.
It would also appear that DIV like VLP is a challenge to treat. Only one of our patients was able to achieve control with topical corticosteroids with all others requiring systemic treatments.
In summary, VLP can present with signs and symptoms mimicking DIV. In patients who have been diagnosed with DIV and demonstrate treatment resistance, an alternative diagnosis of VLP should be considered. The involvement of other body sites, such as oral mucosa, can also help in making the diagnosis of VLP. This subgroup of VLP appears to require systemic treatment in most cases.
None reported.
Ethics approval has been obtained from the Ramsay Health Care Human Research Ethics Committee.
All patients have consented to the inclusion of their cases in this report for journal publication. Consent has been obtained from patients, whose photos are included in this report.
期刊介绍:
Australasian Journal of Dermatology is the official journal of the Australasian College of Dermatologists and the New Zealand Dermatological Society, publishing peer-reviewed, original research articles, reviews and case reports dealing with all aspects of clinical practice and research in dermatology. Clinical presentations, medical and physical therapies and investigations, including dermatopathology and mycology, are covered. Short articles may be published under the headings ‘Signs, Syndromes and Diagnoses’, ‘Dermatopathology Presentation’, ‘Vignettes in Contact Dermatology’, ‘Surgery Corner’ or ‘Letters to the Editor’.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
