Benjamin Enns, Yi Sui, Brenda C. Guerra-Alejos, Lia Humphrey, Micah Piske, Xiao Zang, Susanne Doblecki-Lewis, Daniel J. Feaster, Victoria A. Frye, Elvin H. Geng, Albert Y. Liu, Brandon D. L. Marshall, Scott D. Rhodes, Patrick S. Sullivan, Bohdan Nosyk, the localized economic modelling study group
{"title":"估算美国三个 \"结束艾滋病毒流行 \"辖区以 MSM 为重点的循证干预措施的潜在价值:基于模型的分析。","authors":"Benjamin Enns, Yi Sui, Brenda C. Guerra-Alejos, Lia Humphrey, Micah Piske, Xiao Zang, Susanne Doblecki-Lewis, Daniel J. Feaster, Victoria A. Frye, Elvin H. Geng, Albert Y. Liu, Brandon D. L. Marshall, Scott D. Rhodes, Patrick S. Sullivan, Bohdan Nosyk, the localized economic modelling study group","doi":"10.1002/jia2.26265","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Improving the delivery of existing evidence-based interventions to prevent and diagnose HIV is key to Ending the HIV Epidemic in the United States. Structural barriers in the access and delivery of related health services require municipal or state-level policy changes; however, suboptimal implementation can be addressed directly through interventions designed to improve the reach, effectiveness, adoption or maintenance of available interventions. Our objective was to estimate the cost-effectiveness and potential epidemiological impact of six real-world implementation interventions designed to address these barriers and increase the scale of delivery of interventions for HIV testing and pre-exposure prophylaxis (PrEP) in three US metropolitan areas.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We used a dynamic HIV transmission model calibrated to replicate HIV microepidemics in Atlanta, Los Angeles (LA) and Miami. We identified six implementation interventions designed to improve HIV testing uptake (“Academic detailing for HIV testing,” “CyBER/testing,” “All About Me”) and PrEP uptake/persistence (“Project SLIP,” “PrEPmate,” “PrEP patient navigation”). Our comparator scenario reflected a scale-up of interventions with no additional efforts to mitigate implementation and structural barriers. We accounted for potential heterogeneity in population-level effectiveness across jurisdictions. We sustained implementation interventions over a 10-year period and evaluated HIV acquisitions averted, costs, quality-adjusted life years and incremental cost-effectiveness ratios over a 20-year time horizon (2023–2042).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Across jurisdictions, implementation interventions to improve the scale of HIV testing were most cost-effective in Atlanta and LA (CyBER/testing cost-saving and All About Me cost-effective), while interventions for PrEP were most cost-effective in Miami (two of three were cost-saving). We estimated that the most impactful HIV testing intervention, CyBER/testing, was projected to avert 111 (95% credible interval: 110–111), 230 (228–233) and 101 (101–103) acquisitions over 20 years in Atlanta, LA and Miami, respectively. The most impactful implementation intervention to improve PrEP engagement, PrEPmate, averted an estimated 936 (929–943), 860 (853–867) and 2152 (2127–2178) acquisitions over 20 years, in Atlanta, LA and Miami, respectively.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Our results highlight the potential impact of interventions to enhance the implementation of existing evidence-based interventions for the prevention and diagnosis of HIV.</p>\n </section>\n </div>","PeriodicalId":201,"journal":{"name":"Journal of the International AIDS Society","volume":"27 S1","pages":""},"PeriodicalIF":4.6000,"publicationDate":"2024-07-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jia2.26265","citationCount":"0","resultStr":"{\"title\":\"Estimating the potential value of MSM-focused evidence-based implementation interventions in three Ending the HIV Epidemic jurisdictions in the United States: a model-based analysis\",\"authors\":\"Benjamin Enns, Yi Sui, Brenda C. Guerra-Alejos, Lia Humphrey, Micah Piske, Xiao Zang, Susanne Doblecki-Lewis, Daniel J. Feaster, Victoria A. Frye, Elvin H. Geng, Albert Y. Liu, Brandon D. L. Marshall, Scott D. Rhodes, Patrick S. Sullivan, Bohdan Nosyk, the localized economic modelling study group\",\"doi\":\"10.1002/jia2.26265\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>Improving the delivery of existing evidence-based interventions to prevent and diagnose HIV is key to Ending the HIV Epidemic in the United States. Structural barriers in the access and delivery of related health services require municipal or state-level policy changes; however, suboptimal implementation can be addressed directly through interventions designed to improve the reach, effectiveness, adoption or maintenance of available interventions. Our objective was to estimate the cost-effectiveness and potential epidemiological impact of six real-world implementation interventions designed to address these barriers and increase the scale of delivery of interventions for HIV testing and pre-exposure prophylaxis (PrEP) in three US metropolitan areas.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We used a dynamic HIV transmission model calibrated to replicate HIV microepidemics in Atlanta, Los Angeles (LA) and Miami. We identified six implementation interventions designed to improve HIV testing uptake (“Academic detailing for HIV testing,” “CyBER/testing,” “All About Me”) and PrEP uptake/persistence (“Project SLIP,” “PrEPmate,” “PrEP patient navigation”). Our comparator scenario reflected a scale-up of interventions with no additional efforts to mitigate implementation and structural barriers. We accounted for potential heterogeneity in population-level effectiveness across jurisdictions. We sustained implementation interventions over a 10-year period and evaluated HIV acquisitions averted, costs, quality-adjusted life years and incremental cost-effectiveness ratios over a 20-year time horizon (2023–2042).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Across jurisdictions, implementation interventions to improve the scale of HIV testing were most cost-effective in Atlanta and LA (CyBER/testing cost-saving and All About Me cost-effective), while interventions for PrEP were most cost-effective in Miami (two of three were cost-saving). We estimated that the most impactful HIV testing intervention, CyBER/testing, was projected to avert 111 (95% credible interval: 110–111), 230 (228–233) and 101 (101–103) acquisitions over 20 years in Atlanta, LA and Miami, respectively. The most impactful implementation intervention to improve PrEP engagement, PrEPmate, averted an estimated 936 (929–943), 860 (853–867) and 2152 (2127–2178) acquisitions over 20 years, in Atlanta, LA and Miami, respectively.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Our results highlight the potential impact of interventions to enhance the implementation of existing evidence-based interventions for the prevention and diagnosis of HIV.</p>\\n </section>\\n </div>\",\"PeriodicalId\":201,\"journal\":{\"name\":\"Journal of the International AIDS Society\",\"volume\":\"27 S1\",\"pages\":\"\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2024-07-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jia2.26265\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the International AIDS Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jia2.26265\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the International AIDS Society","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jia2.26265","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
导言:改善现有循证干预措施的实施以预防和诊断艾滋病毒,是结束美国艾滋病毒流行的关键。获取和提供相关医疗服务的结构性障碍需要市政或州一级的政策变革;然而,可以通过旨在改善现有干预措施的覆盖范围、有效性、采用或维持的干预措施直接解决实施效果不佳的问题。我们的目标是估算六个实际实施干预措施的成本效益和潜在流行病学影响,这些干预措施旨在解决这些障碍,并扩大在美国三个大都市地区提供 HIV 检测和暴露前预防(PrEP)干预措施的规模:我们使用了一个动态 HIV 传播模型,该模型经过校准,复制了亚特兰大、洛杉矶和迈阿密的 HIV 微疫情。我们确定了六种实施干预措施,旨在提高 HIV 检测的接受率("HIV 检测学术细化"、"CyBER/检测"、"All About Me")和 PrEP 的接受率/持续率("Project SLIP"、"PrEPmate"、"PrEP 患者导航")。我们的参照方案反映了干预措施的扩大,但没有额外的努力来减少实施和结构性障碍。我们考虑到了各辖区人口层面有效性的潜在异质性。我们在 10 年的时间内持续实施干预措施,并在 20 年的时间跨度内(2023-2042 年)对避免的艾滋病毒感染、成本、质量调整生命年数和增量成本效益比进行了评估:结果:在所有辖区中,亚特兰大和洛杉矶为扩大 HIV 检测规模而采取的干预措施最具成本效益(CyBER/检测可节省成本,All About Me 可节省成本),而迈阿密为 PrEP 采取的干预措施最具成本效益(三项中的两项可节省成本)。我们估计,影响最大的 HIV 检测干预措施 CyBER/testing 预计可在 20 年内分别在亚特兰大、洛杉矶和迈阿密避免 111 例(95% 可信区间:110-111)、230 例(228-233)和 101 例(101-103)死亡。在亚特兰大、洛杉矶和迈阿密,旨在提高 PrEP 参与度的最具影响力的实施干预措施 PrEPmate 预计在 20 年内可分别避免 936 例(929-943)、860 例(853-867)和 2152 例(2127-2178)感染:我们的研究结果凸显了干预措施的潜在影响,即加强现有循证干预措施的实施,以预防和诊断艾滋病。
Estimating the potential value of MSM-focused evidence-based implementation interventions in three Ending the HIV Epidemic jurisdictions in the United States: a model-based analysis
Introduction
Improving the delivery of existing evidence-based interventions to prevent and diagnose HIV is key to Ending the HIV Epidemic in the United States. Structural barriers in the access and delivery of related health services require municipal or state-level policy changes; however, suboptimal implementation can be addressed directly through interventions designed to improve the reach, effectiveness, adoption or maintenance of available interventions. Our objective was to estimate the cost-effectiveness and potential epidemiological impact of six real-world implementation interventions designed to address these barriers and increase the scale of delivery of interventions for HIV testing and pre-exposure prophylaxis (PrEP) in three US metropolitan areas.
Methods
We used a dynamic HIV transmission model calibrated to replicate HIV microepidemics in Atlanta, Los Angeles (LA) and Miami. We identified six implementation interventions designed to improve HIV testing uptake (“Academic detailing for HIV testing,” “CyBER/testing,” “All About Me”) and PrEP uptake/persistence (“Project SLIP,” “PrEPmate,” “PrEP patient navigation”). Our comparator scenario reflected a scale-up of interventions with no additional efforts to mitigate implementation and structural barriers. We accounted for potential heterogeneity in population-level effectiveness across jurisdictions. We sustained implementation interventions over a 10-year period and evaluated HIV acquisitions averted, costs, quality-adjusted life years and incremental cost-effectiveness ratios over a 20-year time horizon (2023–2042).
Results
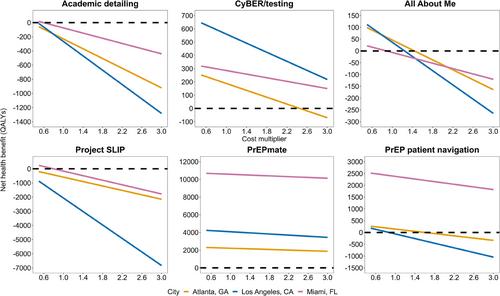
Across jurisdictions, implementation interventions to improve the scale of HIV testing were most cost-effective in Atlanta and LA (CyBER/testing cost-saving and All About Me cost-effective), while interventions for PrEP were most cost-effective in Miami (two of three were cost-saving). We estimated that the most impactful HIV testing intervention, CyBER/testing, was projected to avert 111 (95% credible interval: 110–111), 230 (228–233) and 101 (101–103) acquisitions over 20 years in Atlanta, LA and Miami, respectively. The most impactful implementation intervention to improve PrEP engagement, PrEPmate, averted an estimated 936 (929–943), 860 (853–867) and 2152 (2127–2178) acquisitions over 20 years, in Atlanta, LA and Miami, respectively.
Conclusions
Our results highlight the potential impact of interventions to enhance the implementation of existing evidence-based interventions for the prevention and diagnosis of HIV.
期刊介绍:
The Journal of the International AIDS Society (JIAS) is a peer-reviewed and Open Access journal for the generation and dissemination of evidence from a wide range of disciplines: basic and biomedical sciences; behavioural sciences; epidemiology; clinical sciences; health economics and health policy; operations research and implementation sciences; and social sciences and humanities. Submission of HIV research carried out in low- and middle-income countries is strongly encouraged.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
