{"title":"评估治疗对肾小球滤过率下降影响的临床试验设计。","authors":"","doi":"10.1016/j.kint.2024.06.007","DOIUrl":null,"url":null,"abstract":"<div><p>Glomerular filtration rate (GFR) decline is used as surrogate endpoint for kidney failure. Interventions that reduce chronic kidney disease (CKD) progression often exert acute GFR reductions which differ from their long-term benefits and complicate the estimation of long-term benefit. Here, we assessed the utility of two alternative trial designs (wash-out design and active run-in randomized withdrawal design) that attempt to exclude the impact of acute effects. Post-hoc analyses of two clinical trials that characterized the effect of an intervention with acute reductions in GFR were conducted. The two trials included a wash-out period (EMPA-REG Outcome testing empagliflozin <em>vs</em> placebo) or an active run-in period with a randomized withdrawal (SONAR testing atrasentan <em>vs</em> placebo). We compared the drug effect on GFR decline calculated from the first on-treatment visit to the end of treatment (chronic slope in a standard randomized trial design) with GFR change calculated from randomization to end of wash out, or GFR change from treatment-specific baseline GFR values (GFR at start-of-run-in for placebo and end-of-run-in for atrasentan) until end-of-treatment. The effect of empagliflozin versus placebo on chronic GFR slope was 1.72 (95% confidence interval 1.49-1.94) mL/min/1.73 m<sup>2</sup>/year, similar to total GFR decline from baseline to the end of wash-out period using a linear mixed model 1.64 (1.44-1.85) mL/min/1.73 m<sup>2</sup>/year). The effect of atrasentan versus placebo on chronic GFR slope was 0.72 (0.32-1.11) mL/min/1.73 m<sup>2</sup>/year, similar to total slope from a single slope model when estimated from treatment specific baseline GFR values 0.77 (0.39-1.14) mL/min/1.73 m<sup>2</sup>/year). Statistical power of the two designs outperformed the standard randomized design. Thus, wash-out and active-run-in randomized-withdrawal trial designs are appropriate models to compute treatment effects on GFR decline.</p></div>","PeriodicalId":17801,"journal":{"name":"Kidney international","volume":"106 4","pages":"Pages 723-735"},"PeriodicalIF":12.6000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0085253824004496/pdfft?md5=6386bb62493eba201488dee7b2bf5eec&pid=1-s2.0-S0085253824004496-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Clinical trial designs to assess treatment effects on glomerular filtration rate decline\",\"authors\":\"\",\"doi\":\"10.1016/j.kint.2024.06.007\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>Glomerular filtration rate (GFR) decline is used as surrogate endpoint for kidney failure. Interventions that reduce chronic kidney disease (CKD) progression often exert acute GFR reductions which differ from their long-term benefits and complicate the estimation of long-term benefit. Here, we assessed the utility of two alternative trial designs (wash-out design and active run-in randomized withdrawal design) that attempt to exclude the impact of acute effects. Post-hoc analyses of two clinical trials that characterized the effect of an intervention with acute reductions in GFR were conducted. The two trials included a wash-out period (EMPA-REG Outcome testing empagliflozin <em>vs</em> placebo) or an active run-in period with a randomized withdrawal (SONAR testing atrasentan <em>vs</em> placebo). We compared the drug effect on GFR decline calculated from the first on-treatment visit to the end of treatment (chronic slope in a standard randomized trial design) with GFR change calculated from randomization to end of wash out, or GFR change from treatment-specific baseline GFR values (GFR at start-of-run-in for placebo and end-of-run-in for atrasentan) until end-of-treatment. The effect of empagliflozin versus placebo on chronic GFR slope was 1.72 (95% confidence interval 1.49-1.94) mL/min/1.73 m<sup>2</sup>/year, similar to total GFR decline from baseline to the end of wash-out period using a linear mixed model 1.64 (1.44-1.85) mL/min/1.73 m<sup>2</sup>/year). The effect of atrasentan versus placebo on chronic GFR slope was 0.72 (0.32-1.11) mL/min/1.73 m<sup>2</sup>/year, similar to total slope from a single slope model when estimated from treatment specific baseline GFR values 0.77 (0.39-1.14) mL/min/1.73 m<sup>2</sup>/year). Statistical power of the two designs outperformed the standard randomized design. Thus, wash-out and active-run-in randomized-withdrawal trial designs are appropriate models to compute treatment effects on GFR decline.</p></div>\",\"PeriodicalId\":17801,\"journal\":{\"name\":\"Kidney international\",\"volume\":\"106 4\",\"pages\":\"Pages 723-735\"},\"PeriodicalIF\":12.6000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S0085253824004496/pdfft?md5=6386bb62493eba201488dee7b2bf5eec&pid=1-s2.0-S0085253824004496-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Kidney international\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0085253824004496\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney international","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0085253824004496","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
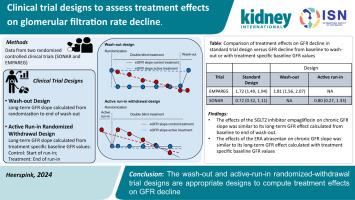
肾小球滤过率(GFR)下降被用作肾衰竭的替代终点。减少慢性肾脏病(CKD)进展的干预措施通常会使肾小球滤过率急性下降,这与其长期益处不同,也使长期益处的评估变得复杂。在此,我们评估了试图排除急性效应影响的两种替代试验设计(冲出设计和积极跑步随机撤出设计)的实用性。我们对两项临床试验的效果进行了事后分析,这两项试验的特点是干预措施会导致 GFR 急性下降。这两项试验包括一个冲出期(EMPAREG-Outcome 试验:安帕格列嗪与安慰剂对比)或一个随机停药的积极运行期(SONAR 试验:阿曲生坦与安慰剂对比)。我们比较了从首次接受治疗到治疗结束(标准随机试验设计中的慢性效应)所计算的药物对GFR下降的影响,以及从随机化到退出治疗结束所计算的GFR变化,或从治疗特定基线GFR值(安慰剂为运行开始时的GFR,阿曲生坦为运行结束时的GFR)到治疗结束的GFR变化。与安慰剂相比,empagliflozin对慢性GFR斜率的影响为1.72(95%置信区间为1.49-1.94)毫升/分钟/1.73平方米/年,与使用线性混合模型计算的从基线到冲洗期结束的GFR总下降率1.64(1.44-1.85)毫升/分钟/1.73平方米/年相似。)阿曲生坦与安慰剂相比对慢性 GFR 斜率的影响为 0.72 (0.32-1.11) mL/min/1.73m2 /年,与根据治疗特定基线 GFR 值估算的单一斜率模型总斜率 0.77 (0.39-1.14) mL/min/1.73m2 /年相似。)两种设计的统计功率优于标准随机设计。因此,"冲出 "和 "主动-运行-输入 "随机-退出试验设计是计算治疗对 GFR 下降影响的合适模型。
Clinical trial designs to assess treatment effects on glomerular filtration rate decline
Glomerular filtration rate (GFR) decline is used as surrogate endpoint for kidney failure. Interventions that reduce chronic kidney disease (CKD) progression often exert acute GFR reductions which differ from their long-term benefits and complicate the estimation of long-term benefit. Here, we assessed the utility of two alternative trial designs (wash-out design and active run-in randomized withdrawal design) that attempt to exclude the impact of acute effects. Post-hoc analyses of two clinical trials that characterized the effect of an intervention with acute reductions in GFR were conducted. The two trials included a wash-out period (EMPA-REG Outcome testing empagliflozin vs placebo) or an active run-in period with a randomized withdrawal (SONAR testing atrasentan vs placebo). We compared the drug effect on GFR decline calculated from the first on-treatment visit to the end of treatment (chronic slope in a standard randomized trial design) with GFR change calculated from randomization to end of wash out, or GFR change from treatment-specific baseline GFR values (GFR at start-of-run-in for placebo and end-of-run-in for atrasentan) until end-of-treatment. The effect of empagliflozin versus placebo on chronic GFR slope was 1.72 (95% confidence interval 1.49-1.94) mL/min/1.73 m2/year, similar to total GFR decline from baseline to the end of wash-out period using a linear mixed model 1.64 (1.44-1.85) mL/min/1.73 m2/year). The effect of atrasentan versus placebo on chronic GFR slope was 0.72 (0.32-1.11) mL/min/1.73 m2/year, similar to total slope from a single slope model when estimated from treatment specific baseline GFR values 0.77 (0.39-1.14) mL/min/1.73 m2/year). Statistical power of the two designs outperformed the standard randomized design. Thus, wash-out and active-run-in randomized-withdrawal trial designs are appropriate models to compute treatment effects on GFR decline.
期刊介绍:
Kidney International (KI), the official journal of the International Society of Nephrology, is led by Dr. Pierre Ronco (Paris, France) and stands as one of nephrology's most cited and esteemed publications worldwide.
KI provides exceptional benefits for both readers and authors, featuring highly cited original articles, focused reviews, cutting-edge imaging techniques, and lively discussions on controversial topics.
The journal is dedicated to kidney research, serving researchers, clinical investigators, and practicing nephrologists.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
