Marian Y Girgis, Eman Mahfouz, Alshaimaa Abdellatif, Farah Taha, Walaa ElNaggar
{"title":"两例难治性肌阵挛性癫痫患者的大脑叶酸转运缺陷。","authors":"Marian Y Girgis, Eman Mahfouz, Alshaimaa Abdellatif, Farah Taha, Walaa ElNaggar","doi":"10.14581/jer.24005","DOIUrl":null,"url":null,"abstract":"<p><p>Cerebral folate transport deficiency due to folate receptor 1 gene (FOLR1) gene mutation results from impaired folate transport across the blood: choroidplexus: cerebrospinal fluid (CSF) barrier. This leads to low CSF 5-methyltetrahydrofolate, the active folate metabolite. We are reporting two children with this treatable cerebral folate transport deficiency. Eight years and 9-month-old female presented with delayed milestones followed by regression, seizures, and intention tremors. On examination child had microcephaly, generalized hypotonia, hyperreflexia, unsteady gait, and incoordination. Magnetic resonance imaging (MRI) of brain revealed dilated ventricular system and cerebellar atrophy. Computed tomography (CT) of brain showed brain calcifications. Whole exome sequencing was finally performed, revealing homozygous nonsense pathogenic variant in FOLR1 gene in exon 3 c.C382T p.R128W, confirming the diagnosis of cerebral folate deficiency. Twelve-year-old female child presented with global developmental delay since birth, myoclonic jerks and cognitive regression. Child had generalized hypotonia and hyperreflexia. Her coordination was markedly affected with intention tremors andunbalanced gait. CT brain showed bilateral basal ganglia and periventricular calcifications with brain atrophic changes. MRI brain showed a prominent cerebellar folia with mild brain atrophic changes. Genetic testing showed a homozygous pathogenic variant was identified in FOLR1 C.327_328 delinsAC, p.Cys109Ter. Both patients were started on intramuscular folinic acid injections with a decrease in seizure frequency. However, their seizures did not stop completely due to late initiation of therapy. In conclusion, cerebral folate transport deficiency should be suspected in every child with global developmental delay, intractable myoclonic epilepsy, ataxia with neuroimaging suggesting cerebellar atrophy and brain calcifications. Response to folinic acid supplementation is partial if diagnosed late and treatment initiation is delayed.</p>","PeriodicalId":73741,"journal":{"name":"Journal of epilepsy research","volume":"14 1","pages":"29-36"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11227922/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cerebral Folate Transport Deficiency in 2 Cases with Intractable Myoclonic Epilepsy.\",\"authors\":\"Marian Y Girgis, Eman Mahfouz, Alshaimaa Abdellatif, Farah Taha, Walaa ElNaggar\",\"doi\":\"10.14581/jer.24005\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Cerebral folate transport deficiency due to folate receptor 1 gene (FOLR1) gene mutation results from impaired folate transport across the blood: choroidplexus: cerebrospinal fluid (CSF) barrier. This leads to low CSF 5-methyltetrahydrofolate, the active folate metabolite. We are reporting two children with this treatable cerebral folate transport deficiency. Eight years and 9-month-old female presented with delayed milestones followed by regression, seizures, and intention tremors. On examination child had microcephaly, generalized hypotonia, hyperreflexia, unsteady gait, and incoordination. Magnetic resonance imaging (MRI) of brain revealed dilated ventricular system and cerebellar atrophy. Computed tomography (CT) of brain showed brain calcifications. Whole exome sequencing was finally performed, revealing homozygous nonsense pathogenic variant in FOLR1 gene in exon 3 c.C382T p.R128W, confirming the diagnosis of cerebral folate deficiency. Twelve-year-old female child presented with global developmental delay since birth, myoclonic jerks and cognitive regression. Child had generalized hypotonia and hyperreflexia. Her coordination was markedly affected with intention tremors andunbalanced gait. CT brain showed bilateral basal ganglia and periventricular calcifications with brain atrophic changes. MRI brain showed a prominent cerebellar folia with mild brain atrophic changes. Genetic testing showed a homozygous pathogenic variant was identified in FOLR1 C.327_328 delinsAC, p.Cys109Ter. Both patients were started on intramuscular folinic acid injections with a decrease in seizure frequency. However, their seizures did not stop completely due to late initiation of therapy. In conclusion, cerebral folate transport deficiency should be suspected in every child with global developmental delay, intractable myoclonic epilepsy, ataxia with neuroimaging suggesting cerebellar atrophy and brain calcifications. Response to folinic acid supplementation is partial if diagnosed late and treatment initiation is delayed.</p>\",\"PeriodicalId\":73741,\"journal\":{\"name\":\"Journal of epilepsy research\",\"volume\":\"14 1\",\"pages\":\"29-36\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-06-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11227922/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of epilepsy research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14581/jer.24005\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of epilepsy research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14581/jer.24005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Cerebral Folate Transport Deficiency in 2 Cases with Intractable Myoclonic Epilepsy.
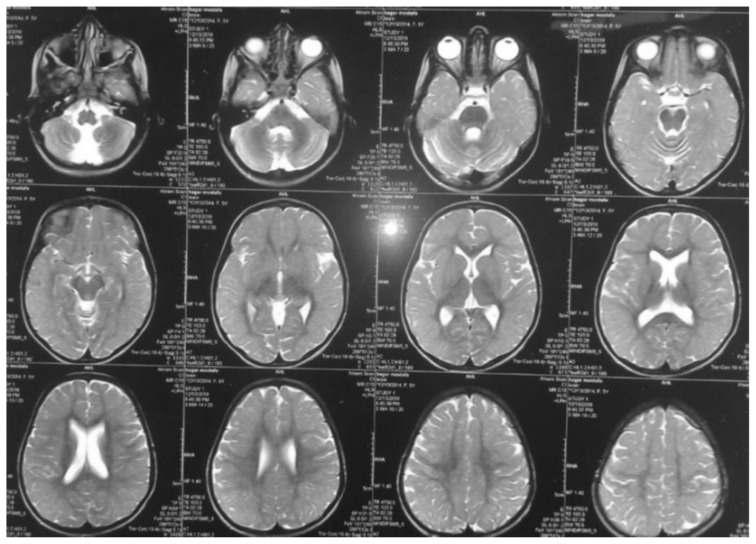
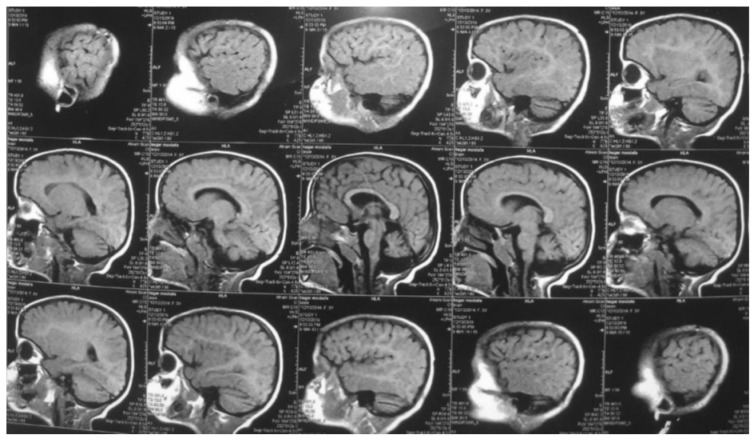
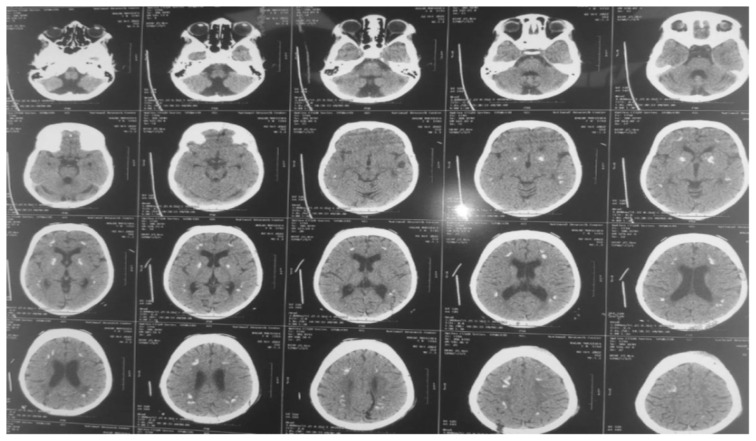
Cerebral folate transport deficiency due to folate receptor 1 gene (FOLR1) gene mutation results from impaired folate transport across the blood: choroidplexus: cerebrospinal fluid (CSF) barrier. This leads to low CSF 5-methyltetrahydrofolate, the active folate metabolite. We are reporting two children with this treatable cerebral folate transport deficiency. Eight years and 9-month-old female presented with delayed milestones followed by regression, seizures, and intention tremors. On examination child had microcephaly, generalized hypotonia, hyperreflexia, unsteady gait, and incoordination. Magnetic resonance imaging (MRI) of brain revealed dilated ventricular system and cerebellar atrophy. Computed tomography (CT) of brain showed brain calcifications. Whole exome sequencing was finally performed, revealing homozygous nonsense pathogenic variant in FOLR1 gene in exon 3 c.C382T p.R128W, confirming the diagnosis of cerebral folate deficiency. Twelve-year-old female child presented with global developmental delay since birth, myoclonic jerks and cognitive regression. Child had generalized hypotonia and hyperreflexia. Her coordination was markedly affected with intention tremors andunbalanced gait. CT brain showed bilateral basal ganglia and periventricular calcifications with brain atrophic changes. MRI brain showed a prominent cerebellar folia with mild brain atrophic changes. Genetic testing showed a homozygous pathogenic variant was identified in FOLR1 C.327_328 delinsAC, p.Cys109Ter. Both patients were started on intramuscular folinic acid injections with a decrease in seizure frequency. However, their seizures did not stop completely due to late initiation of therapy. In conclusion, cerebral folate transport deficiency should be suspected in every child with global developmental delay, intractable myoclonic epilepsy, ataxia with neuroimaging suggesting cerebellar atrophy and brain calcifications. Response to folinic acid supplementation is partial if diagnosed late and treatment initiation is delayed.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
