Ianis Doomun, Daphné Doomun, Sara Schukraft, Diego Arroyo, Selma T Cook, Tibor Huwyler, Jean-Jacques Goy, Jean-Christophe Stauffer, Mario Togni, Serban Puricel, Stéphane Cook
{"title":"经皮冠状动脉介入治疗后 HAS-BLED 和 HEMORR2HAGES 出血风险评分的预测价值。","authors":"Ianis Doomun, Daphné Doomun, Sara Schukraft, Diego Arroyo, Selma T Cook, Tibor Huwyler, Jean-Jacques Goy, Jean-Christophe Stauffer, Mario Togni, Serban Puricel, Stéphane Cook","doi":"10.14503/THIJ-23-8267","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Various scoring systems have been developed to assess the risk of bleeding in medical settings. HAS-BLED and HEMORR2HAGES risk scores are commonly used to estimate bleeding risk in patients receiving anticoagulation for atrial fibrillation, but data on their predictive value in patients undergoing percutaneous coronary intervention (PCI) are limited.</p><p><strong>Methods: </strong>This study evaluated and compared the predictive abilities of the HAS-BLED and HEMORR2HAGES bleeding risk scores in all-comer patients undergoing PCI. The PARIS score, specifically designed for patients undergoing PCI, was used as a comparator. The scores were calculated at baseline and compared with the occurrence of events during a 2-year clinical follow-up period. Between 2015 and 2017, all consecutive patients undergoing PCI we re prospectively enrolled and divided into risk tertiles based on bleeding risk scores. The primary end points were hierarchical major bleeding events, defined by Bleeding Academic Research Consortium types 3 through 5, and patient-oriented composite end points according to Bleeding Academic Research Consortium classification, which were assessed during the 2-year follow-up period.</p><p><strong>Results: </strong>A total of 1,080 patients completed the follow-up period. Two years after index, 189 patients (17.5%) had experienced any bleeding, with 48 events (4.4%) classified as Bleeding Academic Research Consortium types 3 to 5. All bleeding risk scores showed statistically significant predictive ability for bleeding events. The HEMORR2HAGES score (C statistic, 0.73) was more effective than the HAS-BLED score (C statistic, 0.66; P = .07) and the PARIS score (C statistic, 0.66; P = .06) in predicting risk of major bleeding. Patients in high-risk bleeding groups also experienced a higher incidence of patient-oriented composite end points.</p><p><strong>Conclusions: </strong>The HEMORR2HAGES, HAS-BLED, and PARIS risk scores exhibited good predictive abilities for bleeding events following PCI. Patients at high risk of bleeding also demonstrated increased ischemic risk and higher mortality during the 2-year follow-up period.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"51 2","pages":""},"PeriodicalIF":0.9000,"publicationDate":"2024-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11233982/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictive Value of HAS-BLED and HEMORR2HAGES Bleeding Risk Scores After Percutaneous Coronary Intervention.\",\"authors\":\"Ianis Doomun, Daphné Doomun, Sara Schukraft, Diego Arroyo, Selma T Cook, Tibor Huwyler, Jean-Jacques Goy, Jean-Christophe Stauffer, Mario Togni, Serban Puricel, Stéphane Cook\",\"doi\":\"10.14503/THIJ-23-8267\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Various scoring systems have been developed to assess the risk of bleeding in medical settings. HAS-BLED and HEMORR2HAGES risk scores are commonly used to estimate bleeding risk in patients receiving anticoagulation for atrial fibrillation, but data on their predictive value in patients undergoing percutaneous coronary intervention (PCI) are limited.</p><p><strong>Methods: </strong>This study evaluated and compared the predictive abilities of the HAS-BLED and HEMORR2HAGES bleeding risk scores in all-comer patients undergoing PCI. The PARIS score, specifically designed for patients undergoing PCI, was used as a comparator. The scores were calculated at baseline and compared with the occurrence of events during a 2-year clinical follow-up period. Between 2015 and 2017, all consecutive patients undergoing PCI we re prospectively enrolled and divided into risk tertiles based on bleeding risk scores. The primary end points were hierarchical major bleeding events, defined by Bleeding Academic Research Consortium types 3 through 5, and patient-oriented composite end points according to Bleeding Academic Research Consortium classification, which were assessed during the 2-year follow-up period.</p><p><strong>Results: </strong>A total of 1,080 patients completed the follow-up period. Two years after index, 189 patients (17.5%) had experienced any bleeding, with 48 events (4.4%) classified as Bleeding Academic Research Consortium types 3 to 5. All bleeding risk scores showed statistically significant predictive ability for bleeding events. The HEMORR2HAGES score (C statistic, 0.73) was more effective than the HAS-BLED score (C statistic, 0.66; P = .07) and the PARIS score (C statistic, 0.66; P = .06) in predicting risk of major bleeding. Patients in high-risk bleeding groups also experienced a higher incidence of patient-oriented composite end points.</p><p><strong>Conclusions: </strong>The HEMORR2HAGES, HAS-BLED, and PARIS risk scores exhibited good predictive abilities for bleeding events following PCI. Patients at high risk of bleeding also demonstrated increased ischemic risk and higher mortality during the 2-year follow-up period.</p>\",\"PeriodicalId\":48680,\"journal\":{\"name\":\"Texas Heart Institute Journal\",\"volume\":\"51 2\",\"pages\":\"\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-07-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11233982/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Texas Heart Institute Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14503/THIJ-23-8267\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-23-8267","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Predictive Value of HAS-BLED and HEMORR2HAGES Bleeding Risk Scores After Percutaneous Coronary Intervention.
Background: Various scoring systems have been developed to assess the risk of bleeding in medical settings. HAS-BLED and HEMORR2HAGES risk scores are commonly used to estimate bleeding risk in patients receiving anticoagulation for atrial fibrillation, but data on their predictive value in patients undergoing percutaneous coronary intervention (PCI) are limited.
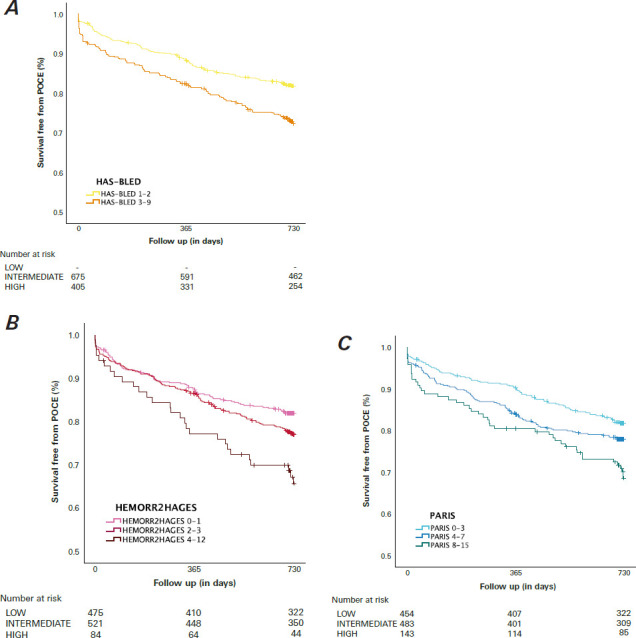
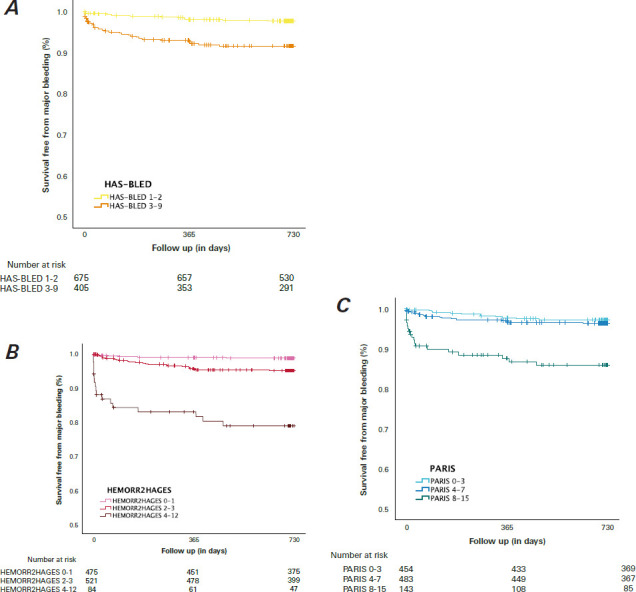
Methods: This study evaluated and compared the predictive abilities of the HAS-BLED and HEMORR2HAGES bleeding risk scores in all-comer patients undergoing PCI. The PARIS score, specifically designed for patients undergoing PCI, was used as a comparator. The scores were calculated at baseline and compared with the occurrence of events during a 2-year clinical follow-up period. Between 2015 and 2017, all consecutive patients undergoing PCI we re prospectively enrolled and divided into risk tertiles based on bleeding risk scores. The primary end points were hierarchical major bleeding events, defined by Bleeding Academic Research Consortium types 3 through 5, and patient-oriented composite end points according to Bleeding Academic Research Consortium classification, which were assessed during the 2-year follow-up period.
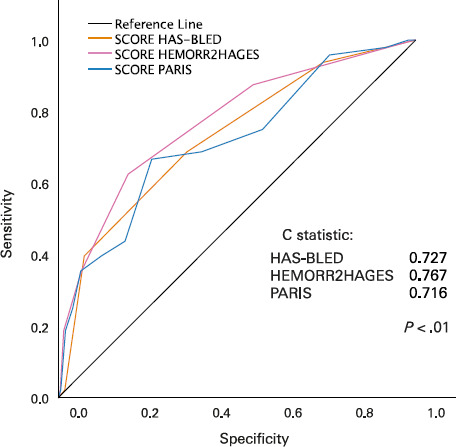
Results: A total of 1,080 patients completed the follow-up period. Two years after index, 189 patients (17.5%) had experienced any bleeding, with 48 events (4.4%) classified as Bleeding Academic Research Consortium types 3 to 5. All bleeding risk scores showed statistically significant predictive ability for bleeding events. The HEMORR2HAGES score (C statistic, 0.73) was more effective than the HAS-BLED score (C statistic, 0.66; P = .07) and the PARIS score (C statistic, 0.66; P = .06) in predicting risk of major bleeding. Patients in high-risk bleeding groups also experienced a higher incidence of patient-oriented composite end points.
Conclusions: The HEMORR2HAGES, HAS-BLED, and PARIS risk scores exhibited good predictive abilities for bleeding events following PCI. Patients at high risk of bleeding also demonstrated increased ischemic risk and higher mortality during the 2-year follow-up period.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
