Riccardo Bomben, Antonella Zucchetto, Roberta Laureana, Annalisa Chiarenza, Jacopo Olivieri, Erika Tissino, Francesca M. Rossi, Filippo Vit, Tamara Bittolo, Robel Papotti, Federico Pozzo, Annalisa Gaglio, Massimo Degan, Jerry Polesel, Roberto Marasca, Andrea Visentin, Riccardo Moia, Idanna Innocenti, Candida Vitale, Roberta Murru, Marzia Varettoni, Agostino Tafuri, Francesco Zaja, Massimiliano Postorino, Enrica A. Martino, Adalgisa Condoluci, Davide Rossi, Antonio Cuneo, Francesco Di Raimondo, Paolo Sportoletti, Ilaria Del Giudice, Robin Foà, Francesca R. Mauro, Marta Coscia, Luca Laurenti, Gianluca Gaidano, Livio Trentin, Maria I. Del Principe, Massimo Gentile, Valter Gattei
{"title":"CD49d表达被纳入预测伊布替尼治疗慢性淋巴细胞白血病患者预后的修订4因素模型:多中心真实世界经验。","authors":"Riccardo Bomben, Antonella Zucchetto, Roberta Laureana, Annalisa Chiarenza, Jacopo Olivieri, Erika Tissino, Francesca M. Rossi, Filippo Vit, Tamara Bittolo, Robel Papotti, Federico Pozzo, Annalisa Gaglio, Massimo Degan, Jerry Polesel, Roberto Marasca, Andrea Visentin, Riccardo Moia, Idanna Innocenti, Candida Vitale, Roberta Murru, Marzia Varettoni, Agostino Tafuri, Francesco Zaja, Massimiliano Postorino, Enrica A. Martino, Adalgisa Condoluci, Davide Rossi, Antonio Cuneo, Francesco Di Raimondo, Paolo Sportoletti, Ilaria Del Giudice, Robin Foà, Francesca R. Mauro, Marta Coscia, Luca Laurenti, Gianluca Gaidano, Livio Trentin, Maria I. Del Principe, Massimo Gentile, Valter Gattei","doi":"10.1002/hem3.128","DOIUrl":null,"url":null,"abstract":"<p>Chronic lymphocytic leukemia (CLL) is a malignancy of mature clonal B lymphocytes that accumulate in blood, bone marrow, and lymphoid tissues.<span><sup>1</sup></span> One of the most important key players in the pathobiology and progression of CLL is the B-cell receptor (BCR) whose activation supports growth and survival of CLL cells.<span><sup>2</sup></span> For this reason, the use of Bruton's tyrosine kinase inhibitors (BTKi) including ibrutinib emerged as one of the most effective treatment options for both naïve (TN) and relapsed/refractory (RR) CLL.<span><sup>2</sup></span> Treatment with BTKi often results in an increase blood lymphocytosis driven by the release of cells from lymph nodes due to impaired interaction with the microenvironment.<span><sup>2-4</sup></span> One of the key molecules of these interactions is the integrin VLA-4 which mediates both cell–cell and cell–matrix interactions playing a crucial role in the retention of CLL cells in tissue-sites thus protecting them from proapoptotic signal.<span><sup>3, 5-7</sup></span> In keeping with these observations, high expression of the VLA-4 integrin alpha chain CD49d (≥30% positive cells), or expression of CD49d according to a bimodal pattern (i.e., concurrent CD49d-positive and CD49d-negative subpopulations, irrespective of the 30% cutoff) identifies CLL cases with reduced recirculation lymphocytosis, inferior nodal response, and shorter progression-free survival (PFS) in the ibrutinib setting.<span><sup>4, 5</sup></span></p><p>In addition to CD49d evaluation, a 4-factor model has been proposed to identify patients at high risk of treatment failure and death during ibrutinib therapy, afterward validated in real-world, which included the TN/RR status, the levels of β2-microglobulin (β2M) and lactate dehydrogenase (LDH) serum concentration, and the TP53 disruption status.<span><sup>8, 9</sup></span> In this context, as well as in other clinical studies on CLL, the TP53 disruption category includes CLL cases with either concurrent TP53 mutation and deletion, or only one of the lesions.<span><sup>1, 8, 9</sup></span> Recently, the prognostic impact of TP53 disruption in ibrutinib-treated CLL has been refined by demonstrating that only cases with the concomitant presence of TP53 deletion and mutations, did not gain maximum benefit from this therapy.<span><sup>10, 11</sup></span></p><p>The aim of this study is to integrate these observations in a comprehensive scoring system for a better management of ibrutinib-treated patients.</p><p>The study is a retrospective/multicenter analysis of 401 CLL patients treated with ibrutinib in the current clinical practice (12/2013–03/2022; approvals IRB-05-2010/IRB-05-2015; CRO Aviano). All CLL cases were characterized for CD49d expression, as reported previously.<span><sup>4-7, 12</sup></span> TP53 disruption was simultaneously evaluated by FISH (17p deletion, del17p) and next-generation sequencing (<i>TP53</i> mutations), as reported.<span><sup>10, 12</sup></span> PFS was calculated from the date of ibrutinib initiation to progression and/or death (death for OS) or last follow-up. Among 401 patients (282 aged ≥65 years at ibrutinib start), 112 died and 169 progressed after median follow-up of 29.9 months (95% confidence interval [CI]: 26.7–34.1 months) and 26.5 months (95% CI: 23.8–29.6 months) from ibrutinib start, respectively. See Supporting Information S1: Table S1 for further details. The canonical 4-factor prediction model was computed as reported<span><sup>8</sup></span>: <i>TP53</i> aberration (del17p and/or <i>TP53</i> mutations) 1 point, >0 prior treatment, 1 point, LDH > 250 U/L, 1 point, β2M ≥ 5 mg/L, 1 point). Patients were stratified into low-risk (score 0-1), intermediate-risk (score 2), high-risk (score 3-4) groups.<span><sup>8</sup></span></p><p>Applying this model we were able to identify 111 low-risk, 160 intermediate-risk, and 130 high-risk cases.<span><sup>8, 9</sup></span> Accordingly, low-risk patients presented a significant longer PFS (median 75.0 months) than patients in the intermediate-risk (median 52.1 months; <i>p</i> = 0.0082) and high-risk groups (median 32.9 months; <i>p</i> < 0.0001, Supporting Information S1: Figure S1A). Low-risk patients also presented a significant longer OS (median 81.7 months) than patients in the intermediate-risk and high-risk groups (<i>p</i> = 0.0131, and <i>p</i> = 0.0010, respectively), while no significant differences were found between intermediate-risk (median 72.8 months), and high-risk patients (median 71.0 months, <i>p</i> = 0.2611, Supporting Information S1: Figure S1B).</p><p>Based on previous findings on the clinical impact of <i>TP53</i> disruption in the ibrutinib setting,<span><sup>10, 11</sup></span> we developed a modified 4-factor model by considering only patients with a concomitant <i>TP53</i> deletion and mutation as <i>TP53</i> disrupted (<i>n</i> = 91; Supporting Information S1: Table S1). Moreover, in keeping with a previous report,<span><sup>13</sup></span> as no difference in PFS and/or OS was found between untreated (<i>n</i> = 57) and 1-line prior treated patients (<i>n</i> = 155; <i>p</i> = 0.6514 or <i>p</i> = 0.8005, respectively; Supporting Information S1: Figure S2AB), these two groups were combined (<i>n</i> = 212) and separated from patients with >1 line prior therapy (<i>n</i> = 189; Supporting Information S1: Table S1). Therefore, one point was assigned to patients with concomitant <i>TP53</i> deletion and mutation, and patients treated with >1 line of prior therapy.<span><sup>8</sup></span> Conversely, the cutoffs for β2M and LDH, also confirmed in our series (Supporting Information S1: Figure S1C and S1D), were maintained as in the original 4-factor study.<span><sup>8</sup></span></p><p>Accordingly, in this modified 4-factor model, 215 low-risk patients presented significantly longer PFS (median 67.9 months) than 108 intermediate-risk (median 47.2 months; <i>p</i> = 0.0017), and 78 high-risk patients (median 20.2 months; <i>p</i> < 0.0001; Figure 1A). The latter model outperformed the canonical 4-factor (C-indices 0.646, 95% CI: 0.604–0.688, vs. 0.628, 95% CI: 0.586–0.670; <i>p</i> < 0.0001). The data were even more evident in the OS setting where C-index for the canonical 4-factor (0.616) was significantly inferior than C-index for the modified 4-factor (0.639; <i>p</i> < 0.0001; Figures S1B and 1B); low-risk patients had significant longer OS (median 82.5 months) than intermediate-risk (median 81.2 months; <i>p</i> = 0.0362), and high-risk (median 51.5 months; <i>p</i> < 0.0001) patients (Figure 1B). Circumscribing the analysis to patients with 0–1 lines of prior therapy, again high-risk patients experienced a shorter PFS than low-risk and intermediate-risk patients (<i>p</i> = 0.0007, and <i>p</i> = 0.0327, respectively; Supporting Information S1: Figure S3A).</p><p>In our cohort, CD49d-high CLL cases (expression ≥30% and/or bimodal, <i>n</i> = 268) had shorter PFS and OS intervals (<i>p</i> = 0.0014 and <i>p</i> = 0.0003, respectively) than CD49d-low cases (<i>n</i> = 133; Figure 1CD). As shown in Supporting Information S1: Table S2, CD49d remained an independent prognostic factor for PFS (<i>p</i> = 0.0232) and OS (<i>p</i> = 0.0038) in multivariable models adjusted with the inclusion of the modified 4-factor intermediate-risk (<i>p</i> = 0.0033, <i>PFS; p</i> = 0.0498, <i>OS</i>) and high-risk (<i>p</i> < 0.0001, <i>PFS; p</i> = 0.0012, <i>OS</i>) groups. We then re-analyzed the individual parameters of the modified 4-factor score together with CD49d expression. According to novel multivariable analyses, LDH was excluded as an independent predictor in favor of CD49d expression (PFS, <i>p</i> = 0.0068; OS, <i>p</i> = 0.0015; Table 1 and Supporting Information S1: Table S2). Consistently, bootstrapping analyses, selected CD49d (PFS, 72.2%; OS, 73.1%) more frequently compared to LDH (PFS, 39.4%; OS, 43.2%) (Table 1 and Supporting Information S1: Table S2).</p><p>According to these results, a novel 4-factor model excluding LDH data in favor of CD49d expression data (4-factor-CD49d) identified 45 scored 0, 137 scored 1, 141 scored 2, 65 scored 3, and 13 scored 4 patients. Based on PFS data, patients with score 0 and 1 presented similar PFS intervals with no significant differences (<i>p</i> = 0.7328); similar behavior was observed for patients with scores 3 and 4 (<i>p</i> = 0.7877) who presented the worst outcome, while cases with score 2, showing intermediate outcomes, differed significantly from all other scores (Supporting Information S1: Figure S4A). Patients were then stratified into three groups with significantly different risk for PFS: score 0-1, low-risk (<i>n</i> = 182); score 2, intermediate-risk (<i>n</i> = 140); score 3-4, high-risk (<i>n</i> = 79; Figure 1E). The inclusion of CD49d into this novel 4-factor model improved its PFS prediction capability (C-index = 0.668, 95% CI: 0.627–0.709; <i>p</i> < 0.0001 vs. both the canonical 4-factor and the 4-factor-modified). Similar results were obtained when considering OS as clinical readout (Figure 1F; C-index = 0.670, 95% CI: 0.621–0.719; <i>p</i> < 0.0001 vs. both the canonical 4-factor and the 4-factor-modified). Focusing only on patients with 0-1 prior lines of therapies, high-risk patients (<i>n</i> = 14) presented significantly shorter PFS than intermediate-risk (<i>n</i> = 55) and low-risk (<i>n</i> = 143) cases (<i>p</i> = 0.0083, and <i>p</i> < 0.0001; respectively; Supporting Information S1: Figure S3B).</p><p>In this scenario, we can speculate that CLL cells with the concomitant presence of the integrin VLA-4, which can promote the retention of CLL cells at tissue sites through binding to its specific ligands,<span><sup>3, 4</sup></span> and <i>TP53</i> disruption, itself responsible for genetic instability,<span><sup>14</sup></span> may be particularly prone to survive/proliferate and accumulate genetic lesions possibly responsible for resistance to ibrutinib. Consistently, the concomitant presence of <i>TP53</i> disruption and high CD49d expression selected a subgroup of patient with a particularly high risk of progression, even when compared with cases with <i>TP53</i> disruption or CD49d expression alone (Supporting Information S1: Figure S4B).</p><p>Although CD49d is not routinely tested and is not recommended by the iwCLL guidelines,<span><sup>1</sup></span> it turned out to be a biomarker that can improve prognostic stratification of patients for both PFS and OS.<span><sup>4, 5</sup></span> In this regard, the C-indices of models that included CD49d approached values of 0.7, a threshold considered necessary to confer utility at the individual patient level.<span><sup>15</sup></span></p><p>This scoring model, generated from patients treated with ibrutinib, should be confirmed in the context of second generation BTKi. Based on the stratification proposed here, patients in the high-risk group could be considered for combination therapies and/or enrollment in clinical trials. Further validation in independent cohorts is needed.</p><p>Riccardo Bomben designed the study, interpreted data, and wrote the manuscript. Antonella Zucchetto, Erika Tissino, Francesca M. Rossi, Filippo Vit, Tamara Bittolo, Robel Papotti, Federico Pozzo, Annalisa Gaglio, Massimo Degan performed and interpreted molecular studies, and contributed to data interpretation. Jerry Polesel performed statistical analyses. Roberta Laureana, Annalisa Chiarenza, Jacopo Olivieri, Roberto Marasca, Andrea Visentin, Riccardo Moia, Idanna Innocenti, Candida Vitale, Roberta Murru, Marzia Varettoni, Agostino Tafuri, Francesco Zaja, Massimiliano Postorino, Enrica A. Martino, Adalgisa Condoluci, Davide Rossi, Antonio Cuneo, Francesco Di Raimondo, Paolo Sportoletti, Ilaria Del Giudice, Robin Foà, Francesca R. Mauro, Marta Coscia, Luca Laurenti, Gianluca Gaidano, Livio Trentin, Maria I. Del Principe, Massimo Gentile collected clinical data and contributed to data interpretation. Valter Gattei designed the study, interpreted data, and wrote the manuscript.</p><p>The authors declare no conflict of interest.</p><p>The present study is supported in part by: Associazione Italiana Ricerca Cancro (AIRC), Investigator Grant IG-21687; PNRR-MAD-2022-12375673 (Next Generation EU, M6/C2_CALL 2022), Italian Ministry of Health, Rome, Italy; Ministero della Salute Ricerca Corrente; Associazione Italiana contro le Leucemie, linfomi e mielomi (AIL), Venezia Section, Italy; “5 × 1000 Intramural Program”, Centro di Riferimento Oncologico, Aviano, Italy; Italian Ministry of Health 5×1000 funds 2013, 2015, 2016.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 7","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2024-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11247362/pdf/","citationCount":"0","resultStr":"{\"title\":\"CD49d expression is included in a revised 4-factor model predicting outcome in patients with chronic lymphocytic leukemia treated with ibrutinib: A multicenter real-world experience\",\"authors\":\"Riccardo Bomben, Antonella Zucchetto, Roberta Laureana, Annalisa Chiarenza, Jacopo Olivieri, Erika Tissino, Francesca M. Rossi, Filippo Vit, Tamara Bittolo, Robel Papotti, Federico Pozzo, Annalisa Gaglio, Massimo Degan, Jerry Polesel, Roberto Marasca, Andrea Visentin, Riccardo Moia, Idanna Innocenti, Candida Vitale, Roberta Murru, Marzia Varettoni, Agostino Tafuri, Francesco Zaja, Massimiliano Postorino, Enrica A. Martino, Adalgisa Condoluci, Davide Rossi, Antonio Cuneo, Francesco Di Raimondo, Paolo Sportoletti, Ilaria Del Giudice, Robin Foà, Francesca R. Mauro, Marta Coscia, Luca Laurenti, Gianluca Gaidano, Livio Trentin, Maria I. Del Principe, Massimo Gentile, Valter Gattei\",\"doi\":\"10.1002/hem3.128\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Chronic lymphocytic leukemia (CLL) is a malignancy of mature clonal B lymphocytes that accumulate in blood, bone marrow, and lymphoid tissues.<span><sup>1</sup></span> One of the most important key players in the pathobiology and progression of CLL is the B-cell receptor (BCR) whose activation supports growth and survival of CLL cells.<span><sup>2</sup></span> For this reason, the use of Bruton's tyrosine kinase inhibitors (BTKi) including ibrutinib emerged as one of the most effective treatment options for both naïve (TN) and relapsed/refractory (RR) CLL.<span><sup>2</sup></span> Treatment with BTKi often results in an increase blood lymphocytosis driven by the release of cells from lymph nodes due to impaired interaction with the microenvironment.<span><sup>2-4</sup></span> One of the key molecules of these interactions is the integrin VLA-4 which mediates both cell–cell and cell–matrix interactions playing a crucial role in the retention of CLL cells in tissue-sites thus protecting them from proapoptotic signal.<span><sup>3, 5-7</sup></span> In keeping with these observations, high expression of the VLA-4 integrin alpha chain CD49d (≥30% positive cells), or expression of CD49d according to a bimodal pattern (i.e., concurrent CD49d-positive and CD49d-negative subpopulations, irrespective of the 30% cutoff) identifies CLL cases with reduced recirculation lymphocytosis, inferior nodal response, and shorter progression-free survival (PFS) in the ibrutinib setting.<span><sup>4, 5</sup></span></p><p>In addition to CD49d evaluation, a 4-factor model has been proposed to identify patients at high risk of treatment failure and death during ibrutinib therapy, afterward validated in real-world, which included the TN/RR status, the levels of β2-microglobulin (β2M) and lactate dehydrogenase (LDH) serum concentration, and the TP53 disruption status.<span><sup>8, 9</sup></span> In this context, as well as in other clinical studies on CLL, the TP53 disruption category includes CLL cases with either concurrent TP53 mutation and deletion, or only one of the lesions.<span><sup>1, 8, 9</sup></span> Recently, the prognostic impact of TP53 disruption in ibrutinib-treated CLL has been refined by demonstrating that only cases with the concomitant presence of TP53 deletion and mutations, did not gain maximum benefit from this therapy.<span><sup>10, 11</sup></span></p><p>The aim of this study is to integrate these observations in a comprehensive scoring system for a better management of ibrutinib-treated patients.</p><p>The study is a retrospective/multicenter analysis of 401 CLL patients treated with ibrutinib in the current clinical practice (12/2013–03/2022; approvals IRB-05-2010/IRB-05-2015; CRO Aviano). All CLL cases were characterized for CD49d expression, as reported previously.<span><sup>4-7, 12</sup></span> TP53 disruption was simultaneously evaluated by FISH (17p deletion, del17p) and next-generation sequencing (<i>TP53</i> mutations), as reported.<span><sup>10, 12</sup></span> PFS was calculated from the date of ibrutinib initiation to progression and/or death (death for OS) or last follow-up. Among 401 patients (282 aged ≥65 years at ibrutinib start), 112 died and 169 progressed after median follow-up of 29.9 months (95% confidence interval [CI]: 26.7–34.1 months) and 26.5 months (95% CI: 23.8–29.6 months) from ibrutinib start, respectively. See Supporting Information S1: Table S1 for further details. The canonical 4-factor prediction model was computed as reported<span><sup>8</sup></span>: <i>TP53</i> aberration (del17p and/or <i>TP53</i> mutations) 1 point, >0 prior treatment, 1 point, LDH > 250 U/L, 1 point, β2M ≥ 5 mg/L, 1 point). Patients were stratified into low-risk (score 0-1), intermediate-risk (score 2), high-risk (score 3-4) groups.<span><sup>8</sup></span></p><p>Applying this model we were able to identify 111 low-risk, 160 intermediate-risk, and 130 high-risk cases.<span><sup>8, 9</sup></span> Accordingly, low-risk patients presented a significant longer PFS (median 75.0 months) than patients in the intermediate-risk (median 52.1 months; <i>p</i> = 0.0082) and high-risk groups (median 32.9 months; <i>p</i> < 0.0001, Supporting Information S1: Figure S1A). Low-risk patients also presented a significant longer OS (median 81.7 months) than patients in the intermediate-risk and high-risk groups (<i>p</i> = 0.0131, and <i>p</i> = 0.0010, respectively), while no significant differences were found between intermediate-risk (median 72.8 months), and high-risk patients (median 71.0 months, <i>p</i> = 0.2611, Supporting Information S1: Figure S1B).</p><p>Based on previous findings on the clinical impact of <i>TP53</i> disruption in the ibrutinib setting,<span><sup>10, 11</sup></span> we developed a modified 4-factor model by considering only patients with a concomitant <i>TP53</i> deletion and mutation as <i>TP53</i> disrupted (<i>n</i> = 91; Supporting Information S1: Table S1). Moreover, in keeping with a previous report,<span><sup>13</sup></span> as no difference in PFS and/or OS was found between untreated (<i>n</i> = 57) and 1-line prior treated patients (<i>n</i> = 155; <i>p</i> = 0.6514 or <i>p</i> = 0.8005, respectively; Supporting Information S1: Figure S2AB), these two groups were combined (<i>n</i> = 212) and separated from patients with >1 line prior therapy (<i>n</i> = 189; Supporting Information S1: Table S1). Therefore, one point was assigned to patients with concomitant <i>TP53</i> deletion and mutation, and patients treated with >1 line of prior therapy.<span><sup>8</sup></span> Conversely, the cutoffs for β2M and LDH, also confirmed in our series (Supporting Information S1: Figure S1C and S1D), were maintained as in the original 4-factor study.<span><sup>8</sup></span></p><p>Accordingly, in this modified 4-factor model, 215 low-risk patients presented significantly longer PFS (median 67.9 months) than 108 intermediate-risk (median 47.2 months; <i>p</i> = 0.0017), and 78 high-risk patients (median 20.2 months; <i>p</i> < 0.0001; Figure 1A). The latter model outperformed the canonical 4-factor (C-indices 0.646, 95% CI: 0.604–0.688, vs. 0.628, 95% CI: 0.586–0.670; <i>p</i> < 0.0001). The data were even more evident in the OS setting where C-index for the canonical 4-factor (0.616) was significantly inferior than C-index for the modified 4-factor (0.639; <i>p</i> < 0.0001; Figures S1B and 1B); low-risk patients had significant longer OS (median 82.5 months) than intermediate-risk (median 81.2 months; <i>p</i> = 0.0362), and high-risk (median 51.5 months; <i>p</i> < 0.0001) patients (Figure 1B). Circumscribing the analysis to patients with 0–1 lines of prior therapy, again high-risk patients experienced a shorter PFS than low-risk and intermediate-risk patients (<i>p</i> = 0.0007, and <i>p</i> = 0.0327, respectively; Supporting Information S1: Figure S3A).</p><p>In our cohort, CD49d-high CLL cases (expression ≥30% and/or bimodal, <i>n</i> = 268) had shorter PFS and OS intervals (<i>p</i> = 0.0014 and <i>p</i> = 0.0003, respectively) than CD49d-low cases (<i>n</i> = 133; Figure 1CD). As shown in Supporting Information S1: Table S2, CD49d remained an independent prognostic factor for PFS (<i>p</i> = 0.0232) and OS (<i>p</i> = 0.0038) in multivariable models adjusted with the inclusion of the modified 4-factor intermediate-risk (<i>p</i> = 0.0033, <i>PFS; p</i> = 0.0498, <i>OS</i>) and high-risk (<i>p</i> < 0.0001, <i>PFS; p</i> = 0.0012, <i>OS</i>) groups. We then re-analyzed the individual parameters of the modified 4-factor score together with CD49d expression. According to novel multivariable analyses, LDH was excluded as an independent predictor in favor of CD49d expression (PFS, <i>p</i> = 0.0068; OS, <i>p</i> = 0.0015; Table 1 and Supporting Information S1: Table S2). Consistently, bootstrapping analyses, selected CD49d (PFS, 72.2%; OS, 73.1%) more frequently compared to LDH (PFS, 39.4%; OS, 43.2%) (Table 1 and Supporting Information S1: Table S2).</p><p>According to these results, a novel 4-factor model excluding LDH data in favor of CD49d expression data (4-factor-CD49d) identified 45 scored 0, 137 scored 1, 141 scored 2, 65 scored 3, and 13 scored 4 patients. Based on PFS data, patients with score 0 and 1 presented similar PFS intervals with no significant differences (<i>p</i> = 0.7328); similar behavior was observed for patients with scores 3 and 4 (<i>p</i> = 0.7877) who presented the worst outcome, while cases with score 2, showing intermediate outcomes, differed significantly from all other scores (Supporting Information S1: Figure S4A). Patients were then stratified into three groups with significantly different risk for PFS: score 0-1, low-risk (<i>n</i> = 182); score 2, intermediate-risk (<i>n</i> = 140); score 3-4, high-risk (<i>n</i> = 79; Figure 1E). The inclusion of CD49d into this novel 4-factor model improved its PFS prediction capability (C-index = 0.668, 95% CI: 0.627–0.709; <i>p</i> < 0.0001 vs. both the canonical 4-factor and the 4-factor-modified). Similar results were obtained when considering OS as clinical readout (Figure 1F; C-index = 0.670, 95% CI: 0.621–0.719; <i>p</i> < 0.0001 vs. both the canonical 4-factor and the 4-factor-modified). Focusing only on patients with 0-1 prior lines of therapies, high-risk patients (<i>n</i> = 14) presented significantly shorter PFS than intermediate-risk (<i>n</i> = 55) and low-risk (<i>n</i> = 143) cases (<i>p</i> = 0.0083, and <i>p</i> < 0.0001; respectively; Supporting Information S1: Figure S3B).</p><p>In this scenario, we can speculate that CLL cells with the concomitant presence of the integrin VLA-4, which can promote the retention of CLL cells at tissue sites through binding to its specific ligands,<span><sup>3, 4</sup></span> and <i>TP53</i> disruption, itself responsible for genetic instability,<span><sup>14</sup></span> may be particularly prone to survive/proliferate and accumulate genetic lesions possibly responsible for resistance to ibrutinib. Consistently, the concomitant presence of <i>TP53</i> disruption and high CD49d expression selected a subgroup of patient with a particularly high risk of progression, even when compared with cases with <i>TP53</i> disruption or CD49d expression alone (Supporting Information S1: Figure S4B).</p><p>Although CD49d is not routinely tested and is not recommended by the iwCLL guidelines,<span><sup>1</sup></span> it turned out to be a biomarker that can improve prognostic stratification of patients for both PFS and OS.<span><sup>4, 5</sup></span> In this regard, the C-indices of models that included CD49d approached values of 0.7, a threshold considered necessary to confer utility at the individual patient level.<span><sup>15</sup></span></p><p>This scoring model, generated from patients treated with ibrutinib, should be confirmed in the context of second generation BTKi. Based on the stratification proposed here, patients in the high-risk group could be considered for combination therapies and/or enrollment in clinical trials. Further validation in independent cohorts is needed.</p><p>Riccardo Bomben designed the study, interpreted data, and wrote the manuscript. Antonella Zucchetto, Erika Tissino, Francesca M. Rossi, Filippo Vit, Tamara Bittolo, Robel Papotti, Federico Pozzo, Annalisa Gaglio, Massimo Degan performed and interpreted molecular studies, and contributed to data interpretation. Jerry Polesel performed statistical analyses. Roberta Laureana, Annalisa Chiarenza, Jacopo Olivieri, Roberto Marasca, Andrea Visentin, Riccardo Moia, Idanna Innocenti, Candida Vitale, Roberta Murru, Marzia Varettoni, Agostino Tafuri, Francesco Zaja, Massimiliano Postorino, Enrica A. Martino, Adalgisa Condoluci, Davide Rossi, Antonio Cuneo, Francesco Di Raimondo, Paolo Sportoletti, Ilaria Del Giudice, Robin Foà, Francesca R. Mauro, Marta Coscia, Luca Laurenti, Gianluca Gaidano, Livio Trentin, Maria I. Del Principe, Massimo Gentile collected clinical data and contributed to data interpretation. Valter Gattei designed the study, interpreted data, and wrote the manuscript.</p><p>The authors declare no conflict of interest.</p><p>The present study is supported in part by: Associazione Italiana Ricerca Cancro (AIRC), Investigator Grant IG-21687; PNRR-MAD-2022-12375673 (Next Generation EU, M6/C2_CALL 2022), Italian Ministry of Health, Rome, Italy; Ministero della Salute Ricerca Corrente; Associazione Italiana contro le Leucemie, linfomi e mielomi (AIL), Venezia Section, Italy; “5 × 1000 Intramural Program”, Centro di Riferimento Oncologico, Aviano, Italy; Italian Ministry of Health 5×1000 funds 2013, 2015, 2016.</p>\",\"PeriodicalId\":12982,\"journal\":{\"name\":\"HemaSphere\",\"volume\":\"8 7\",\"pages\":\"\"},\"PeriodicalIF\":14.6000,\"publicationDate\":\"2024-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11247362/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HemaSphere\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hem3.128\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.128","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
CD49d expression is included in a revised 4-factor model predicting outcome in patients with chronic lymphocytic leukemia treated with ibrutinib: A multicenter real-world experience
Chronic lymphocytic leukemia (CLL) is a malignancy of mature clonal B lymphocytes that accumulate in blood, bone marrow, and lymphoid tissues.1 One of the most important key players in the pathobiology and progression of CLL is the B-cell receptor (BCR) whose activation supports growth and survival of CLL cells.2 For this reason, the use of Bruton's tyrosine kinase inhibitors (BTKi) including ibrutinib emerged as one of the most effective treatment options for both naïve (TN) and relapsed/refractory (RR) CLL.2 Treatment with BTKi often results in an increase blood lymphocytosis driven by the release of cells from lymph nodes due to impaired interaction with the microenvironment.2-4 One of the key molecules of these interactions is the integrin VLA-4 which mediates both cell–cell and cell–matrix interactions playing a crucial role in the retention of CLL cells in tissue-sites thus protecting them from proapoptotic signal.3, 5-7 In keeping with these observations, high expression of the VLA-4 integrin alpha chain CD49d (≥30% positive cells), or expression of CD49d according to a bimodal pattern (i.e., concurrent CD49d-positive and CD49d-negative subpopulations, irrespective of the 30% cutoff) identifies CLL cases with reduced recirculation lymphocytosis, inferior nodal response, and shorter progression-free survival (PFS) in the ibrutinib setting.4, 5
In addition to CD49d evaluation, a 4-factor model has been proposed to identify patients at high risk of treatment failure and death during ibrutinib therapy, afterward validated in real-world, which included the TN/RR status, the levels of β2-microglobulin (β2M) and lactate dehydrogenase (LDH) serum concentration, and the TP53 disruption status.8, 9 In this context, as well as in other clinical studies on CLL, the TP53 disruption category includes CLL cases with either concurrent TP53 mutation and deletion, or only one of the lesions.1, 8, 9 Recently, the prognostic impact of TP53 disruption in ibrutinib-treated CLL has been refined by demonstrating that only cases with the concomitant presence of TP53 deletion and mutations, did not gain maximum benefit from this therapy.10, 11
The aim of this study is to integrate these observations in a comprehensive scoring system for a better management of ibrutinib-treated patients.
The study is a retrospective/multicenter analysis of 401 CLL patients treated with ibrutinib in the current clinical practice (12/2013–03/2022; approvals IRB-05-2010/IRB-05-2015; CRO Aviano). All CLL cases were characterized for CD49d expression, as reported previously.4-7, 12 TP53 disruption was simultaneously evaluated by FISH (17p deletion, del17p) and next-generation sequencing (TP53 mutations), as reported.10, 12 PFS was calculated from the date of ibrutinib initiation to progression and/or death (death for OS) or last follow-up. Among 401 patients (282 aged ≥65 years at ibrutinib start), 112 died and 169 progressed after median follow-up of 29.9 months (95% confidence interval [CI]: 26.7–34.1 months) and 26.5 months (95% CI: 23.8–29.6 months) from ibrutinib start, respectively. See Supporting Information S1: Table S1 for further details. The canonical 4-factor prediction model was computed as reported8: TP53 aberration (del17p and/or TP53 mutations) 1 point, >0 prior treatment, 1 point, LDH > 250 U/L, 1 point, β2M ≥ 5 mg/L, 1 point). Patients were stratified into low-risk (score 0-1), intermediate-risk (score 2), high-risk (score 3-4) groups.8
Applying this model we were able to identify 111 low-risk, 160 intermediate-risk, and 130 high-risk cases.8, 9 Accordingly, low-risk patients presented a significant longer PFS (median 75.0 months) than patients in the intermediate-risk (median 52.1 months; p = 0.0082) and high-risk groups (median 32.9 months; p < 0.0001, Supporting Information S1: Figure S1A). Low-risk patients also presented a significant longer OS (median 81.7 months) than patients in the intermediate-risk and high-risk groups (p = 0.0131, and p = 0.0010, respectively), while no significant differences were found between intermediate-risk (median 72.8 months), and high-risk patients (median 71.0 months, p = 0.2611, Supporting Information S1: Figure S1B).
Based on previous findings on the clinical impact of TP53 disruption in the ibrutinib setting,10, 11 we developed a modified 4-factor model by considering only patients with a concomitant TP53 deletion and mutation as TP53 disrupted (n = 91; Supporting Information S1: Table S1). Moreover, in keeping with a previous report,13 as no difference in PFS and/or OS was found between untreated (n = 57) and 1-line prior treated patients (n = 155; p = 0.6514 or p = 0.8005, respectively; Supporting Information S1: Figure S2AB), these two groups were combined (n = 212) and separated from patients with >1 line prior therapy (n = 189; Supporting Information S1: Table S1). Therefore, one point was assigned to patients with concomitant TP53 deletion and mutation, and patients treated with >1 line of prior therapy.8 Conversely, the cutoffs for β2M and LDH, also confirmed in our series (Supporting Information S1: Figure S1C and S1D), were maintained as in the original 4-factor study.8
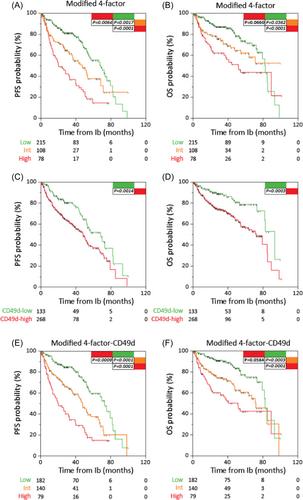
Accordingly, in this modified 4-factor model, 215 low-risk patients presented significantly longer PFS (median 67.9 months) than 108 intermediate-risk (median 47.2 months; p = 0.0017), and 78 high-risk patients (median 20.2 months; p < 0.0001; Figure 1A). The latter model outperformed the canonical 4-factor (C-indices 0.646, 95% CI: 0.604–0.688, vs. 0.628, 95% CI: 0.586–0.670; p < 0.0001). The data were even more evident in the OS setting where C-index for the canonical 4-factor (0.616) was significantly inferior than C-index for the modified 4-factor (0.639; p < 0.0001; Figures S1B and 1B); low-risk patients had significant longer OS (median 82.5 months) than intermediate-risk (median 81.2 months; p = 0.0362), and high-risk (median 51.5 months; p < 0.0001) patients (Figure 1B). Circumscribing the analysis to patients with 0–1 lines of prior therapy, again high-risk patients experienced a shorter PFS than low-risk and intermediate-risk patients (p = 0.0007, and p = 0.0327, respectively; Supporting Information S1: Figure S3A).
In our cohort, CD49d-high CLL cases (expression ≥30% and/or bimodal, n = 268) had shorter PFS and OS intervals (p = 0.0014 and p = 0.0003, respectively) than CD49d-low cases (n = 133; Figure 1CD). As shown in Supporting Information S1: Table S2, CD49d remained an independent prognostic factor for PFS (p = 0.0232) and OS (p = 0.0038) in multivariable models adjusted with the inclusion of the modified 4-factor intermediate-risk (p = 0.0033, PFS; p = 0.0498, OS) and high-risk (p < 0.0001, PFS; p = 0.0012, OS) groups. We then re-analyzed the individual parameters of the modified 4-factor score together with CD49d expression. According to novel multivariable analyses, LDH was excluded as an independent predictor in favor of CD49d expression (PFS, p = 0.0068; OS, p = 0.0015; Table 1 and Supporting Information S1: Table S2). Consistently, bootstrapping analyses, selected CD49d (PFS, 72.2%; OS, 73.1%) more frequently compared to LDH (PFS, 39.4%; OS, 43.2%) (Table 1 and Supporting Information S1: Table S2).
According to these results, a novel 4-factor model excluding LDH data in favor of CD49d expression data (4-factor-CD49d) identified 45 scored 0, 137 scored 1, 141 scored 2, 65 scored 3, and 13 scored 4 patients. Based on PFS data, patients with score 0 and 1 presented similar PFS intervals with no significant differences (p = 0.7328); similar behavior was observed for patients with scores 3 and 4 (p = 0.7877) who presented the worst outcome, while cases with score 2, showing intermediate outcomes, differed significantly from all other scores (Supporting Information S1: Figure S4A). Patients were then stratified into three groups with significantly different risk for PFS: score 0-1, low-risk (n = 182); score 2, intermediate-risk (n = 140); score 3-4, high-risk (n = 79; Figure 1E). The inclusion of CD49d into this novel 4-factor model improved its PFS prediction capability (C-index = 0.668, 95% CI: 0.627–0.709; p < 0.0001 vs. both the canonical 4-factor and the 4-factor-modified). Similar results were obtained when considering OS as clinical readout (Figure 1F; C-index = 0.670, 95% CI: 0.621–0.719; p < 0.0001 vs. both the canonical 4-factor and the 4-factor-modified). Focusing only on patients with 0-1 prior lines of therapies, high-risk patients (n = 14) presented significantly shorter PFS than intermediate-risk (n = 55) and low-risk (n = 143) cases (p = 0.0083, and p < 0.0001; respectively; Supporting Information S1: Figure S3B).
In this scenario, we can speculate that CLL cells with the concomitant presence of the integrin VLA-4, which can promote the retention of CLL cells at tissue sites through binding to its specific ligands,3, 4 and TP53 disruption, itself responsible for genetic instability,14 may be particularly prone to survive/proliferate and accumulate genetic lesions possibly responsible for resistance to ibrutinib. Consistently, the concomitant presence of TP53 disruption and high CD49d expression selected a subgroup of patient with a particularly high risk of progression, even when compared with cases with TP53 disruption or CD49d expression alone (Supporting Information S1: Figure S4B).
Although CD49d is not routinely tested and is not recommended by the iwCLL guidelines,1 it turned out to be a biomarker that can improve prognostic stratification of patients for both PFS and OS.4, 5 In this regard, the C-indices of models that included CD49d approached values of 0.7, a threshold considered necessary to confer utility at the individual patient level.15
This scoring model, generated from patients treated with ibrutinib, should be confirmed in the context of second generation BTKi. Based on the stratification proposed here, patients in the high-risk group could be considered for combination therapies and/or enrollment in clinical trials. Further validation in independent cohorts is needed.
Riccardo Bomben designed the study, interpreted data, and wrote the manuscript. Antonella Zucchetto, Erika Tissino, Francesca M. Rossi, Filippo Vit, Tamara Bittolo, Robel Papotti, Federico Pozzo, Annalisa Gaglio, Massimo Degan performed and interpreted molecular studies, and contributed to data interpretation. Jerry Polesel performed statistical analyses. Roberta Laureana, Annalisa Chiarenza, Jacopo Olivieri, Roberto Marasca, Andrea Visentin, Riccardo Moia, Idanna Innocenti, Candida Vitale, Roberta Murru, Marzia Varettoni, Agostino Tafuri, Francesco Zaja, Massimiliano Postorino, Enrica A. Martino, Adalgisa Condoluci, Davide Rossi, Antonio Cuneo, Francesco Di Raimondo, Paolo Sportoletti, Ilaria Del Giudice, Robin Foà, Francesca R. Mauro, Marta Coscia, Luca Laurenti, Gianluca Gaidano, Livio Trentin, Maria I. Del Principe, Massimo Gentile collected clinical data and contributed to data interpretation. Valter Gattei designed the study, interpreted data, and wrote the manuscript.
The authors declare no conflict of interest.
The present study is supported in part by: Associazione Italiana Ricerca Cancro (AIRC), Investigator Grant IG-21687; PNRR-MAD-2022-12375673 (Next Generation EU, M6/C2_CALL 2022), Italian Ministry of Health, Rome, Italy; Ministero della Salute Ricerca Corrente; Associazione Italiana contro le Leucemie, linfomi e mielomi (AIL), Venezia Section, Italy; “5 × 1000 Intramural Program”, Centro di Riferimento Oncologico, Aviano, Italy; Italian Ministry of Health 5×1000 funds 2013, 2015, 2016.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
