Marc Edy Pierre, Angélica Viviana Fletcher Prieto, Juliana Rodríguez, Abraham Hernández Blanquisett, Ana Milena Gómez Camacho, Rafael Parra Medina, Lucrecia Mojica Silva, Robinson Fernández, Pedro Hernando Calderón Quiroz
{"title":"哥伦比亚子宫内膜癌分子诊断共识","authors":"Marc Edy Pierre, Angélica Viviana Fletcher Prieto, Juliana Rodríguez, Abraham Hernández Blanquisett, Ana Milena Gómez Camacho, Rafael Parra Medina, Lucrecia Mojica Silva, Robinson Fernández, Pedro Hernando Calderón Quiroz","doi":"10.18597/rcog.4060","DOIUrl":null,"url":null,"abstract":"<p><p>Objective: The Cancer Genome Atlas research program (TCGA) developed the molecular classification for endometrial cancer with prognostic and therapeutic utility, which was replaced by the ProMisE (Proactive Molecular Risk Classifier for Endometrial Cancer) classification by consensus and international guidelines due to its high cost. This article aims to present national recommendations from an expert consensus that allows unification and implementation of the molecular classification for women with endometrial cancer nationwide, with a rational use of resources and technology.\n\nMethods: Consensus of 36 experts in clinical oncology, oncological gynecology, pathology, and genetics, with clinical practice in the national territory. The leader group performed a literature review and structuring of questions rated 1 to 9 points. A modified nominal group technique was used. There was a face-to-face meeting with master presentations, deliberative dialogue, and Google Forms (Google LLC, Mountain View, CA, USA) questionnaire voting with analysis and discussion of responses. The non-consensual responses led to a second round of voting. The final manuscript was finally prepared and revised.\n\nResults: Seven recommendations were formulated integrating the panelist responses based on evidence, but adjusted to the Colombian context and reality.\n\nRecommendation 1. The molecular classification is recommended in all the endometrial cancers using the immunohistochemistry markers as subrogated results from the molecular profile initially proposed in the TCGA classification.\n\nRecommendation 2. The sequential test strategy is recommended, starting with the immunohistochemistry markers (p53, MLH1, MSH 2, MSH6, PMS2) simultaneously in all the patients, defining to request POLE (DNA polymerase epsilon) (if available) according to the risk classification based on the surgical piece.\n\nRecommendation 3. It is recommended, that the gynecologist oncologist should be the one to request the POLE (if available) according to the final pathology report. This test must be requested for all endometrial cancers stage I-II, except in low risk (stage IA low grade endometrioid histology without linfovascular invasion normal p53) and, stages III-IV without residual disease, without affecting the request of subrogated immunohistochemistry molecular markers upon histology.\n\nThe consensus proposes that the POLE is requested after the immunohistochemistry and according to the categories in the risk classification established by the 2020 ESGO/ESTRO/ESP guidelines.\n\nRecommendation 4. It is recommended to perform immunohistochemistry for hormonal receptors for all women with endometrial cancer and the HER2 in patients with p53abn, simultaneously with the others immunohistochemistry markers.\n\nRecommendation 5. It is recommended to perform the immunohistochemistry markers (p53, MLH1, MSH2, MSH6 y PMS2) in an initial endometrial biopsy or curettage when the specimen is adequate and available. In case the initial immunohistochemistry is inconclusive, or there are histological discrepancies between the initial and definitive pathology, it is recommended to repeat the molecular profile in the surgical pathology. The immunohistochemistry markers must be reported in the pathology report according to the CAP (College of American Pathologists) recommendations, independently of the type of sample.\n\nRecommendation 6. It is recommended to perform MLH1 promoter methylation testing in patients who exhibit loss of expression of MLH1 in immunohistochemistry whether it is accompanied or not with loss of expression of PMS2. All the patients with deficient MMR (mismatch repair), should be sent for genetic counseling to rule out Lynch syndrome.\n\nRecommendation 7. It is recommended to consider the molecular classification in addition to the classical histopathological criteria when making adjuvant judgments, as incorporated by the classification of prognostic groups of the 2020 ESGO/ESTRO/ESP guidelines.\n\nConclusions: It is necessary to implement the molecular classification of endometrial cancer in clinical practice in accordance to the Colombian context, due to its prognostic and probably predictive value. This will enable the characterization of the Colombian population in order to offer individualized guided treatments. This is an academic and nonregulatory document.</p>","PeriodicalId":101422,"journal":{"name":"Revista colombiana de obstetricia y ginecologia","volume":"75 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11208073/pdf/","citationCount":"0","resultStr":"{\"title\":\"Colombian consensus for the molecular diagnosis of endometrial cancer\",\"authors\":\"Marc Edy Pierre, Angélica Viviana Fletcher Prieto, Juliana Rodríguez, Abraham Hernández Blanquisett, Ana Milena Gómez Camacho, Rafael Parra Medina, Lucrecia Mojica Silva, Robinson Fernández, Pedro Hernando Calderón Quiroz\",\"doi\":\"10.18597/rcog.4060\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Objective: The Cancer Genome Atlas research program (TCGA) developed the molecular classification for endometrial cancer with prognostic and therapeutic utility, which was replaced by the ProMisE (Proactive Molecular Risk Classifier for Endometrial Cancer) classification by consensus and international guidelines due to its high cost. This article aims to present national recommendations from an expert consensus that allows unification and implementation of the molecular classification for women with endometrial cancer nationwide, with a rational use of resources and technology.\\n\\nMethods: Consensus of 36 experts in clinical oncology, oncological gynecology, pathology, and genetics, with clinical practice in the national territory. The leader group performed a literature review and structuring of questions rated 1 to 9 points. A modified nominal group technique was used. There was a face-to-face meeting with master presentations, deliberative dialogue, and Google Forms (Google LLC, Mountain View, CA, USA) questionnaire voting with analysis and discussion of responses. The non-consensual responses led to a second round of voting. The final manuscript was finally prepared and revised.\\n\\nResults: Seven recommendations were formulated integrating the panelist responses based on evidence, but adjusted to the Colombian context and reality.\\n\\nRecommendation 1. The molecular classification is recommended in all the endometrial cancers using the immunohistochemistry markers as subrogated results from the molecular profile initially proposed in the TCGA classification.\\n\\nRecommendation 2. The sequential test strategy is recommended, starting with the immunohistochemistry markers (p53, MLH1, MSH 2, MSH6, PMS2) simultaneously in all the patients, defining to request POLE (DNA polymerase epsilon) (if available) according to the risk classification based on the surgical piece.\\n\\nRecommendation 3. It is recommended, that the gynecologist oncologist should be the one to request the POLE (if available) according to the final pathology report. This test must be requested for all endometrial cancers stage I-II, except in low risk (stage IA low grade endometrioid histology without linfovascular invasion normal p53) and, stages III-IV without residual disease, without affecting the request of subrogated immunohistochemistry molecular markers upon histology.\\n\\nThe consensus proposes that the POLE is requested after the immunohistochemistry and according to the categories in the risk classification established by the 2020 ESGO/ESTRO/ESP guidelines.\\n\\nRecommendation 4. It is recommended to perform immunohistochemistry for hormonal receptors for all women with endometrial cancer and the HER2 in patients with p53abn, simultaneously with the others immunohistochemistry markers.\\n\\nRecommendation 5. It is recommended to perform the immunohistochemistry markers (p53, MLH1, MSH2, MSH6 y PMS2) in an initial endometrial biopsy or curettage when the specimen is adequate and available. In case the initial immunohistochemistry is inconclusive, or there are histological discrepancies between the initial and definitive pathology, it is recommended to repeat the molecular profile in the surgical pathology. The immunohistochemistry markers must be reported in the pathology report according to the CAP (College of American Pathologists) recommendations, independently of the type of sample.\\n\\nRecommendation 6. It is recommended to perform MLH1 promoter methylation testing in patients who exhibit loss of expression of MLH1 in immunohistochemistry whether it is accompanied or not with loss of expression of PMS2. All the patients with deficient MMR (mismatch repair), should be sent for genetic counseling to rule out Lynch syndrome.\\n\\nRecommendation 7. It is recommended to consider the molecular classification in addition to the classical histopathological criteria when making adjuvant judgments, as incorporated by the classification of prognostic groups of the 2020 ESGO/ESTRO/ESP guidelines.\\n\\nConclusions: It is necessary to implement the molecular classification of endometrial cancer in clinical practice in accordance to the Colombian context, due to its prognostic and probably predictive value. This will enable the characterization of the Colombian population in order to offer individualized guided treatments. This is an academic and nonregulatory document.</p>\",\"PeriodicalId\":101422,\"journal\":{\"name\":\"Revista colombiana de obstetricia y ginecologia\",\"volume\":\"75 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-06-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11208073/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Revista colombiana de obstetricia y ginecologia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.18597/rcog.4060\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista colombiana de obstetricia y ginecologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18597/rcog.4060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Colombian consensus for the molecular diagnosis of endometrial cancer
Objective: The Cancer Genome Atlas research program (TCGA) developed the molecular classification for endometrial cancer with prognostic and therapeutic utility, which was replaced by the ProMisE (Proactive Molecular Risk Classifier for Endometrial Cancer) classification by consensus and international guidelines due to its high cost. This article aims to present national recommendations from an expert consensus that allows unification and implementation of the molecular classification for women with endometrial cancer nationwide, with a rational use of resources and technology.
Methods: Consensus of 36 experts in clinical oncology, oncological gynecology, pathology, and genetics, with clinical practice in the national territory. The leader group performed a literature review and structuring of questions rated 1 to 9 points. A modified nominal group technique was used. There was a face-to-face meeting with master presentations, deliberative dialogue, and Google Forms (Google LLC, Mountain View, CA, USA) questionnaire voting with analysis and discussion of responses. The non-consensual responses led to a second round of voting. The final manuscript was finally prepared and revised.
Results: Seven recommendations were formulated integrating the panelist responses based on evidence, but adjusted to the Colombian context and reality.
Recommendation 1. The molecular classification is recommended in all the endometrial cancers using the immunohistochemistry markers as subrogated results from the molecular profile initially proposed in the TCGA classification.
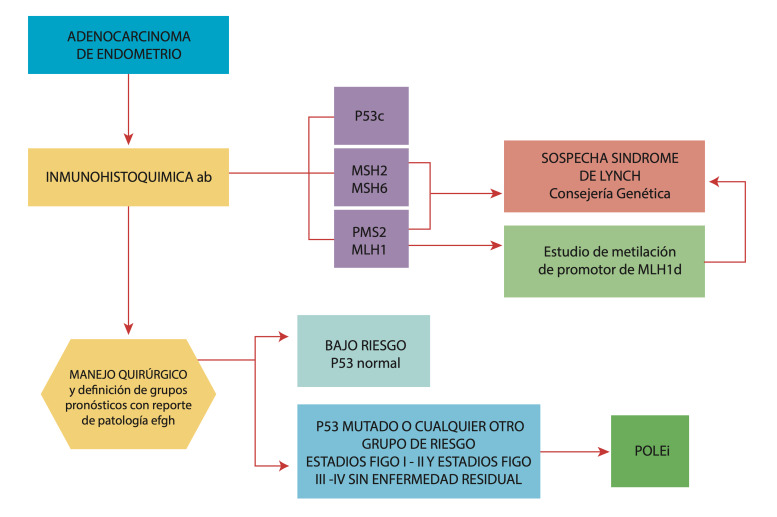
Recommendation 2. The sequential test strategy is recommended, starting with the immunohistochemistry markers (p53, MLH1, MSH 2, MSH6, PMS2) simultaneously in all the patients, defining to request POLE (DNA polymerase epsilon) (if available) according to the risk classification based on the surgical piece.
Recommendation 3. It is recommended, that the gynecologist oncologist should be the one to request the POLE (if available) according to the final pathology report. This test must be requested for all endometrial cancers stage I-II, except in low risk (stage IA low grade endometrioid histology without linfovascular invasion normal p53) and, stages III-IV without residual disease, without affecting the request of subrogated immunohistochemistry molecular markers upon histology.
The consensus proposes that the POLE is requested after the immunohistochemistry and according to the categories in the risk classification established by the 2020 ESGO/ESTRO/ESP guidelines.
Recommendation 4. It is recommended to perform immunohistochemistry for hormonal receptors for all women with endometrial cancer and the HER2 in patients with p53abn, simultaneously with the others immunohistochemistry markers.
Recommendation 5. It is recommended to perform the immunohistochemistry markers (p53, MLH1, MSH2, MSH6 y PMS2) in an initial endometrial biopsy or curettage when the specimen is adequate and available. In case the initial immunohistochemistry is inconclusive, or there are histological discrepancies between the initial and definitive pathology, it is recommended to repeat the molecular profile in the surgical pathology. The immunohistochemistry markers must be reported in the pathology report according to the CAP (College of American Pathologists) recommendations, independently of the type of sample.
Recommendation 6. It is recommended to perform MLH1 promoter methylation testing in patients who exhibit loss of expression of MLH1 in immunohistochemistry whether it is accompanied or not with loss of expression of PMS2. All the patients with deficient MMR (mismatch repair), should be sent for genetic counseling to rule out Lynch syndrome.
Recommendation 7. It is recommended to consider the molecular classification in addition to the classical histopathological criteria when making adjuvant judgments, as incorporated by the classification of prognostic groups of the 2020 ESGO/ESTRO/ESP guidelines.
Conclusions: It is necessary to implement the molecular classification of endometrial cancer in clinical practice in accordance to the Colombian context, due to its prognostic and probably predictive value. This will enable the characterization of the Colombian population in order to offer individualized guided treatments. This is an academic and nonregulatory document.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
