Danielle S. Powell AuD, PhD, Mingche M. J. Wu MSPH, Stephanie Nothelle MD, Jamie M. Smith RN PhD, Kelly Gleason PN, PhD, Esther S. Oh MD, PhD, Hillary D. Lum MD, PhD, Nicholas S. Reed AuD, Jennifer L. Wolff PhD
{"title":"医疗保险年度健康检查:改善医疗系统识别听力损失的机会?","authors":"Danielle S. Powell AuD, PhD, Mingche M. J. Wu MSPH, Stephanie Nothelle MD, Jamie M. Smith RN PhD, Kelly Gleason PN, PhD, Esther S. Oh MD, PhD, Hillary D. Lum MD, PhD, Nicholas S. Reed AuD, Jennifer L. Wolff PhD","doi":"10.1111/jgs.19111","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Hearing loss is prevalent and consequential but under-diagnosed and managed. The Medicare Annual Wellness Visit (AWV) health risk assessment elicits patient-reported hearing concerns but whether such information affects documentation, diagnosis, or referral is unknown.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We use 5 years of electronic medical record (EMR) data (2017–2022) for a sample of 13,776 older primary care patients. We identify the first (index) AWV indication of hearing concerns and existing and subsequent hearing loss EMR diagnoses (visit diagnoses or problem list diagnoses) and audiology referrals. For a 20% random sample of AWV notes (<i>n</i> = 474) we compared hearing loss EMR diagnoses to documentation of (1) hearing concerns, (2) hearing loss/aid use, and (3) referrals for hearing care.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of 3845 (27.9%) older adults who identified hearing concerns (mean age 79.1 years, 57% female, 75% white) 24% had an existing hearing diagnosis recorded. Among 474 patients with AWV clinical notes reviewed, 90 (19%) had an existing hearing loss diagnosis. Clinicians were more likely to document hearing concerns or hearing loss/aid use for those with (vs. without) an existing EMR diagnosis (50.6% vs. 35.9%, <i>p</i> = 0.01; 68.9% vs. 37.5%, <i>p</i> < 0.001, respectively). EMR diagnoses of hearing loss were recorded for no more than 40% of those with indicated hearing concerns. Among those without prior diagnosis 38 (9.9%) received a hearing care referral within 1 month. Subgroup analysis suggest greater likelihood of documenting hearing concerns for patients age 80+ (OR:1.51, 95% confidence interval [CI]: 1.03, 2.19) and decreased likelihood of documenting known hearing loss among patients with more chronic conditions (OR: 0.49, 95% CI: 0.27, 0.9), with no differences observed by race.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Documentation of hearing loss in EMR and AWV clinical notes is limited among older adults with subjective hearing concerns. Systematic support and incorporation of hearing into EMR and clinical notes may increase hearing loss visibility by care teams.</p>\n </section>\n </div>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 10","pages":"3089-3097"},"PeriodicalIF":4.5000,"publicationDate":"2024-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11461099/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Medicare annual wellness visit: An opportunity to improve health system identification of hearing loss?\",\"authors\":\"Danielle S. Powell AuD, PhD, Mingche M. J. Wu MSPH, Stephanie Nothelle MD, Jamie M. Smith RN PhD, Kelly Gleason PN, PhD, Esther S. Oh MD, PhD, Hillary D. Lum MD, PhD, Nicholas S. Reed AuD, Jennifer L. Wolff PhD\",\"doi\":\"10.1111/jgs.19111\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Hearing loss is prevalent and consequential but under-diagnosed and managed. The Medicare Annual Wellness Visit (AWV) health risk assessment elicits patient-reported hearing concerns but whether such information affects documentation, diagnosis, or referral is unknown.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We use 5 years of electronic medical record (EMR) data (2017–2022) for a sample of 13,776 older primary care patients. We identify the first (index) AWV indication of hearing concerns and existing and subsequent hearing loss EMR diagnoses (visit diagnoses or problem list diagnoses) and audiology referrals. For a 20% random sample of AWV notes (<i>n</i> = 474) we compared hearing loss EMR diagnoses to documentation of (1) hearing concerns, (2) hearing loss/aid use, and (3) referrals for hearing care.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Of 3845 (27.9%) older adults who identified hearing concerns (mean age 79.1 years, 57% female, 75% white) 24% had an existing hearing diagnosis recorded. Among 474 patients with AWV clinical notes reviewed, 90 (19%) had an existing hearing loss diagnosis. Clinicians were more likely to document hearing concerns or hearing loss/aid use for those with (vs. without) an existing EMR diagnosis (50.6% vs. 35.9%, <i>p</i> = 0.01; 68.9% vs. 37.5%, <i>p</i> < 0.001, respectively). EMR diagnoses of hearing loss were recorded for no more than 40% of those with indicated hearing concerns. Among those without prior diagnosis 38 (9.9%) received a hearing care referral within 1 month. Subgroup analysis suggest greater likelihood of documenting hearing concerns for patients age 80+ (OR:1.51, 95% confidence interval [CI]: 1.03, 2.19) and decreased likelihood of documenting known hearing loss among patients with more chronic conditions (OR: 0.49, 95% CI: 0.27, 0.9), with no differences observed by race.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Documentation of hearing loss in EMR and AWV clinical notes is limited among older adults with subjective hearing concerns. Systematic support and incorporation of hearing into EMR and clinical notes may increase hearing loss visibility by care teams.</p>\\n </section>\\n </div>\",\"PeriodicalId\":17240,\"journal\":{\"name\":\"Journal of the American Geriatrics Society\",\"volume\":\"72 10\",\"pages\":\"3089-3097\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2024-07-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11461099/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Geriatrics Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19111\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19111","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
The Medicare annual wellness visit: An opportunity to improve health system identification of hearing loss?
Background
Hearing loss is prevalent and consequential but under-diagnosed and managed. The Medicare Annual Wellness Visit (AWV) health risk assessment elicits patient-reported hearing concerns but whether such information affects documentation, diagnosis, or referral is unknown.
Methods
We use 5 years of electronic medical record (EMR) data (2017–2022) for a sample of 13,776 older primary care patients. We identify the first (index) AWV indication of hearing concerns and existing and subsequent hearing loss EMR diagnoses (visit diagnoses or problem list diagnoses) and audiology referrals. For a 20% random sample of AWV notes (n = 474) we compared hearing loss EMR diagnoses to documentation of (1) hearing concerns, (2) hearing loss/aid use, and (3) referrals for hearing care.
Results
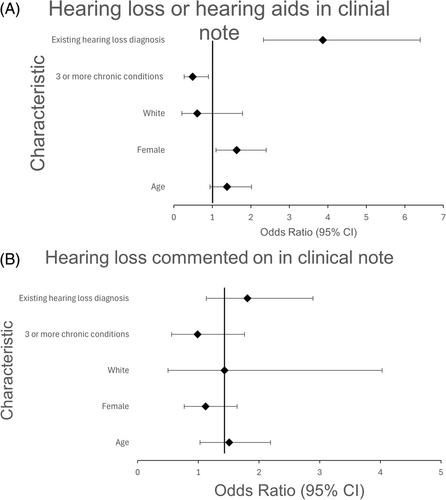
Of 3845 (27.9%) older adults who identified hearing concerns (mean age 79.1 years, 57% female, 75% white) 24% had an existing hearing diagnosis recorded. Among 474 patients with AWV clinical notes reviewed, 90 (19%) had an existing hearing loss diagnosis. Clinicians were more likely to document hearing concerns or hearing loss/aid use for those with (vs. without) an existing EMR diagnosis (50.6% vs. 35.9%, p = 0.01; 68.9% vs. 37.5%, p < 0.001, respectively). EMR diagnoses of hearing loss were recorded for no more than 40% of those with indicated hearing concerns. Among those without prior diagnosis 38 (9.9%) received a hearing care referral within 1 month. Subgroup analysis suggest greater likelihood of documenting hearing concerns for patients age 80+ (OR:1.51, 95% confidence interval [CI]: 1.03, 2.19) and decreased likelihood of documenting known hearing loss among patients with more chronic conditions (OR: 0.49, 95% CI: 0.27, 0.9), with no differences observed by race.
Conclusion
Documentation of hearing loss in EMR and AWV clinical notes is limited among older adults with subjective hearing concerns. Systematic support and incorporation of hearing into EMR and clinical notes may increase hearing loss visibility by care teams.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
