James O. Jordano MD, Eduard E. Vasilevskis MD, MPH, Sandra F. Simmons PhD, Warren D. Taylor MD, MHSc, Andrew A. Monte MD, PhD, Maria C. Duggan MD, MPH, Jin H. Han MD, MSc
{"title":"选择性血清素/血清素-去甲肾上腺素再摄取抑制剂血清浓度与谵妄持续时间的关系。","authors":"James O. Jordano MD, Eduard E. Vasilevskis MD, MPH, Sandra F. Simmons PhD, Warren D. Taylor MD, MHSc, Andrew A. Monte MD, PhD, Maria C. Duggan MD, MPH, Jin H. Han MD, MSc","doi":"10.1111/jgs.19107","DOIUrl":null,"url":null,"abstract":"<p>Delirium is a form of acute brain failure that commonly afflicts older hospitalized patients.<span><sup>1</sup></span> The association between delirium and benzodiazepines is well-documented,<span><sup>2</sup></span> but the association with other psychotropic medication classes is less clear. Using a novel liquid chromatography-mass spectrometry (LC-MS) assay, we observed supratherapeutic psychotropic drug levels (SPDLs) occurred in 17% of delirium cases and were associated with prolonged delirium episodes. Over half of SPDLs were secondary to selective and serotonin-norepinephrine reuptake inhibitors (SSRI/SNRIs),<span><sup>3</sup></span> which are not considered deliriogenic.<span><sup>2</sup></span> Most studies examining SSRI/SNRIs and delirium relied on medication lists, which do not account for SPDLs.<span><sup>4, 5</sup></span> They also did not account for preexisting dementia, which may increase vulnerability to developing delirium, even at nontoxic, therapeutic drug concentrations.<span><sup>4, 5</sup></span> We sought to determine if serum SSRI/SNRI concentrations were associated with prolonged delirium duration in older hospitalized adults and examined if this association was modified by preexisting dementia.</p><p>This was an exploratory analysis of a prospective cohort study.<span><sup>3, 6</sup></span> Patients ≥65 years old who were admitted to the hospital, had serum available for LC-MS measurements, and enrolled within 4 h of emergency department presentation were included. All delirious and a random selection (~17%) of non-delirious patients were enrolled between March 2012 and November 2014.</p><p>Delirium was assessed daily using the modified Brief Confusion Assessment Method (bCAM), which is 82% sensitive and 96% specific for delirium.<span><sup>7</sup></span> Serum SSRI/SNRI drug levels were measured using a LC-MS assay that measured 30+ psychotropic medications (Precera Bioscience, Inc., Franklin, TN). Standardized serum SSRI/SNRI concentrations were calculated by dividing each measurement by the upper limit of normal published in the literature. To establish the validity of our standardization approach, we analyzed standardized serum benzodiazepine concentrations. A patient was considered to have pre-illness dementia if they had: (i) a pre-illness dementia assessment (IQCODE) greater than 3.38,<span><sup>8</sup></span> (ii) documented dementia diagnosis in the medical record, or (iii) prescribed cholinesterase inhibitors prior to admission.</p><p>To determine if standardized serum concentrations of SSRI/SNRIs or benzodiazepines were associated with delirium duration, proportional odds logistic regression was performed adjusting for age, pre-illness dementia, functional status, and depression, comorbidity burden, pre-illness severity, kidney/liver dysfunction, and central nervous system diagnosis.<span><sup>6</sup></span> A standardized serum concentration*pre-illness dementia interaction was incorporated; effect modification was considered present if the <i>p</i>-value was <0.20. Adjusted odds ratios (aORs) with 95% confidence intervals (95% CI) are reported. Statistical analyses were performed on SAS version 9.3 (SAS Institute, Cary, NC).</p><p>Patient characteristics for the 158 patients included in this analysis can be seen in Supplemental Table 1. The median (interquartile range) delirium duration was 3 (2, 5) days. SSRI/SNRIs and benzodiazepines were detected in the sera in 54 (34.2%) and 26 (16.5%) patients, respectively. Of note, five out of 56 (8.9%) had SSRI/SNRIs and eight out of 26 (30.8%) had benzodiazepines detected by LC-MS, but were not listed in the electronic health record.</p><p>As standardized serum concentrations of SSRI/SNRI and benzodiazepines increased, delirium duration also increased (Figure 1). The aOR (95% CI) for the proportional odds logistic regression models evaluating the association between serum SSRI/SNRI and benzodiazepine concentrations and delirium duration are seen in Figure 2. In the adjusted analysis, standardized serum SSRI/SNRI concentrations were significantly associated with longer delirium duration in patients with preexisting dementia only (aOR = 2.4, 95% CI: 1.2, 4.7, <i>p</i>-value for interaction = 0.126). Standardized serum benzodiazepine concentrations were significantly associated with delirium duration, regardless of preexisting dementia status (aOR = 3.1, 95% CI: 1.1, 9.0, <i>p</i>-value for interaction = 0.265).</p><p>We observed that standardized serum SSRI/SNRI concentrations were associated with prolonged delirium duration in older hospitalized adults. The association was more prominent in those with preexisting dementia, who are the most vulnerable to developing delirium. This has multiple possible explanations: SSRI/SNRIs worsen delirium, may represent polypharmacy, serve as markers of advanced dementia with behavioral disturbances, or indicate aging physiology and reduced cognitive reserve. Further work is necessary to elucidate if SSRI/SNRIs have a causative effect on delirium duration. Most SSRI/SNRIs are not considered potentially inappropriate medications by established criteria.<span><sup>9</sup></span> Our study suggests that older patients taking prescribed SSRI/SNRIs with delirium may benefit from serum concentration measurement. If elevated, dose reduction may be considered, especially if the patient has preexisting dementia. Because this was an exploratory analysis, our findings require confirmation.</p><p>We used a novel LC-MS assay to measure serum drug concentrations of psychotropic medications, which is a more accurate method to characterize drug exposure. Studies using medication lists can miss an average of two medications and do not take into account nonadherence.<span><sup>10</sup></span> In our cohort, 9% and 31% of SSRI/SNRIs and benzodiazepines, respectively, were detected in the serum but were not documented in the electronic health record. LC-MS serum drug measurements can also account for toxic serum drug levels, which may lead to delirium and other adverse outcomes. This approach seems valid as standardized serum benzodiazepine concentrations were also associated with prolonged delirium.</p><p>Our study has several limitations. Residual confounding likely exists. We also did not evaluate the effect of SSRI/SNRIs on long-term cognition. A larger prospective cohort study is needed to examine this in older patients.</p><p>JHH designed the original DELINEATE study. JHH designed the exploratory analysis, supervised data collection, and performed the statistical analysis. JOJ, JHH had access to the entire data set. JHH performed the statistical analysis. JOJ, JHH wrote the primary manuscript draft. All authors provided substantial revisions and approved the final manuscript.</p><p>Dr. Jin H. Han and this study were funded by the National Institutes of Health under award number K23AG032355. This study was also supported by the National Center for Research Resources, Grant UL1 RR024975-01, and is now at the National Center for Advancing Translational Sciences, Grant 2 UL1 TR000445-06. Precera Bioscience, Inc, provided the serum drug concentration measurements for this study. Dr. Eduard E. Vasilevskis and Dr. Sandra F. Simmons are supported by the National Institutes of Health under award number R01AG53264. Dr. Jin H. Han, Dr. Eduard E. Vasilevskis, and Dr. Sandra F. Simmons are also supported by the Veteran Affairs Geriatric Research, Education, and Clinical Center (GRECC).</p><p>All authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this manuscript.</p><p>The sponsor had no role in the design of the study, the collection and analysis of the data, or the preparation of the manuscript.</p>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 11","pages":"3594-3597"},"PeriodicalIF":4.5000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11560737/pdf/","citationCount":"0","resultStr":"{\"title\":\"Selective serotonin/serotonin-norepinephrine reuptake inhibitor serum concentrations' association with delirium duration\",\"authors\":\"James O. Jordano MD, Eduard E. Vasilevskis MD, MPH, Sandra F. Simmons PhD, Warren D. Taylor MD, MHSc, Andrew A. Monte MD, PhD, Maria C. Duggan MD, MPH, Jin H. Han MD, MSc\",\"doi\":\"10.1111/jgs.19107\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Delirium is a form of acute brain failure that commonly afflicts older hospitalized patients.<span><sup>1</sup></span> The association between delirium and benzodiazepines is well-documented,<span><sup>2</sup></span> but the association with other psychotropic medication classes is less clear. Using a novel liquid chromatography-mass spectrometry (LC-MS) assay, we observed supratherapeutic psychotropic drug levels (SPDLs) occurred in 17% of delirium cases and were associated with prolonged delirium episodes. Over half of SPDLs were secondary to selective and serotonin-norepinephrine reuptake inhibitors (SSRI/SNRIs),<span><sup>3</sup></span> which are not considered deliriogenic.<span><sup>2</sup></span> Most studies examining SSRI/SNRIs and delirium relied on medication lists, which do not account for SPDLs.<span><sup>4, 5</sup></span> They also did not account for preexisting dementia, which may increase vulnerability to developing delirium, even at nontoxic, therapeutic drug concentrations.<span><sup>4, 5</sup></span> We sought to determine if serum SSRI/SNRI concentrations were associated with prolonged delirium duration in older hospitalized adults and examined if this association was modified by preexisting dementia.</p><p>This was an exploratory analysis of a prospective cohort study.<span><sup>3, 6</sup></span> Patients ≥65 years old who were admitted to the hospital, had serum available for LC-MS measurements, and enrolled within 4 h of emergency department presentation were included. All delirious and a random selection (~17%) of non-delirious patients were enrolled between March 2012 and November 2014.</p><p>Delirium was assessed daily using the modified Brief Confusion Assessment Method (bCAM), which is 82% sensitive and 96% specific for delirium.<span><sup>7</sup></span> Serum SSRI/SNRI drug levels were measured using a LC-MS assay that measured 30+ psychotropic medications (Precera Bioscience, Inc., Franklin, TN). Standardized serum SSRI/SNRI concentrations were calculated by dividing each measurement by the upper limit of normal published in the literature. To establish the validity of our standardization approach, we analyzed standardized serum benzodiazepine concentrations. A patient was considered to have pre-illness dementia if they had: (i) a pre-illness dementia assessment (IQCODE) greater than 3.38,<span><sup>8</sup></span> (ii) documented dementia diagnosis in the medical record, or (iii) prescribed cholinesterase inhibitors prior to admission.</p><p>To determine if standardized serum concentrations of SSRI/SNRIs or benzodiazepines were associated with delirium duration, proportional odds logistic regression was performed adjusting for age, pre-illness dementia, functional status, and depression, comorbidity burden, pre-illness severity, kidney/liver dysfunction, and central nervous system diagnosis.<span><sup>6</sup></span> A standardized serum concentration*pre-illness dementia interaction was incorporated; effect modification was considered present if the <i>p</i>-value was <0.20. Adjusted odds ratios (aORs) with 95% confidence intervals (95% CI) are reported. Statistical analyses were performed on SAS version 9.3 (SAS Institute, Cary, NC).</p><p>Patient characteristics for the 158 patients included in this analysis can be seen in Supplemental Table 1. The median (interquartile range) delirium duration was 3 (2, 5) days. SSRI/SNRIs and benzodiazepines were detected in the sera in 54 (34.2%) and 26 (16.5%) patients, respectively. Of note, five out of 56 (8.9%) had SSRI/SNRIs and eight out of 26 (30.8%) had benzodiazepines detected by LC-MS, but were not listed in the electronic health record.</p><p>As standardized serum concentrations of SSRI/SNRI and benzodiazepines increased, delirium duration also increased (Figure 1). The aOR (95% CI) for the proportional odds logistic regression models evaluating the association between serum SSRI/SNRI and benzodiazepine concentrations and delirium duration are seen in Figure 2. In the adjusted analysis, standardized serum SSRI/SNRI concentrations were significantly associated with longer delirium duration in patients with preexisting dementia only (aOR = 2.4, 95% CI: 1.2, 4.7, <i>p</i>-value for interaction = 0.126). Standardized serum benzodiazepine concentrations were significantly associated with delirium duration, regardless of preexisting dementia status (aOR = 3.1, 95% CI: 1.1, 9.0, <i>p</i>-value for interaction = 0.265).</p><p>We observed that standardized serum SSRI/SNRI concentrations were associated with prolonged delirium duration in older hospitalized adults. The association was more prominent in those with preexisting dementia, who are the most vulnerable to developing delirium. This has multiple possible explanations: SSRI/SNRIs worsen delirium, may represent polypharmacy, serve as markers of advanced dementia with behavioral disturbances, or indicate aging physiology and reduced cognitive reserve. Further work is necessary to elucidate if SSRI/SNRIs have a causative effect on delirium duration. Most SSRI/SNRIs are not considered potentially inappropriate medications by established criteria.<span><sup>9</sup></span> Our study suggests that older patients taking prescribed SSRI/SNRIs with delirium may benefit from serum concentration measurement. If elevated, dose reduction may be considered, especially if the patient has preexisting dementia. Because this was an exploratory analysis, our findings require confirmation.</p><p>We used a novel LC-MS assay to measure serum drug concentrations of psychotropic medications, which is a more accurate method to characterize drug exposure. Studies using medication lists can miss an average of two medications and do not take into account nonadherence.<span><sup>10</sup></span> In our cohort, 9% and 31% of SSRI/SNRIs and benzodiazepines, respectively, were detected in the serum but were not documented in the electronic health record. LC-MS serum drug measurements can also account for toxic serum drug levels, which may lead to delirium and other adverse outcomes. This approach seems valid as standardized serum benzodiazepine concentrations were also associated with prolonged delirium.</p><p>Our study has several limitations. Residual confounding likely exists. We also did not evaluate the effect of SSRI/SNRIs on long-term cognition. A larger prospective cohort study is needed to examine this in older patients.</p><p>JHH designed the original DELINEATE study. JHH designed the exploratory analysis, supervised data collection, and performed the statistical analysis. JOJ, JHH had access to the entire data set. JHH performed the statistical analysis. JOJ, JHH wrote the primary manuscript draft. All authors provided substantial revisions and approved the final manuscript.</p><p>Dr. Jin H. Han and this study were funded by the National Institutes of Health under award number K23AG032355. This study was also supported by the National Center for Research Resources, Grant UL1 RR024975-01, and is now at the National Center for Advancing Translational Sciences, Grant 2 UL1 TR000445-06. Precera Bioscience, Inc, provided the serum drug concentration measurements for this study. Dr. Eduard E. Vasilevskis and Dr. Sandra F. Simmons are supported by the National Institutes of Health under award number R01AG53264. Dr. Jin H. Han, Dr. Eduard E. Vasilevskis, and Dr. Sandra F. Simmons are also supported by the Veteran Affairs Geriatric Research, Education, and Clinical Center (GRECC).</p><p>All authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this manuscript.</p><p>The sponsor had no role in the design of the study, the collection and analysis of the data, or the preparation of the manuscript.</p>\",\"PeriodicalId\":17240,\"journal\":{\"name\":\"Journal of the American Geriatrics Society\",\"volume\":\"72 11\",\"pages\":\"3594-3597\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2024-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11560737/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Geriatrics Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19107\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19107","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
如果药物浓度升高,可以考虑减少剂量,尤其是在患者已经患有痴呆症的情况下。由于这是一项探索性分析,我们的研究结果尚需确认。我们使用了一种新型的 LC-MS 检测方法来测量精神药物的血清药物浓度,这是一种更准确地描述药物暴露特征的方法。10 在我们的队列中,分别有 9% 和 31% 的 SSRI/SNRIs 和苯二氮卓类药物在血清中被检测到,但并未记录在电子健康记录中。LC-MS 血清药物测量还能说明血清中的毒性药物水平,这可能会导致谵妄和其他不良后果。我们的研究有几个局限性。我们的研究存在一些局限性。我们的研究存在一些局限性。我们也没有评估 SSRI/SNRIs 对长期认知能力的影响。我们需要在老年患者中开展更大规模的前瞻性队列研究来研究这一点。JHH设计了探索性分析,监督了数据收集,并进行了统计分析。JOJ、JHH可以访问整个数据集。JHH 进行了统计分析。JOJ、JHH撰写了手稿初稿。所有作者都对稿件进行了实质性修改,并批准了最终稿件。Jin H. Han博士和本研究得到了美国国立卫生研究院(National Institutes of Health)的资助,奖励号为K23AG032355。这项研究还得到了美国国家研究资源中心(National Center for Research Resources)UL1 RR024975-01号基金的支持,目前正在美国国家转化科学促进中心(National Center for Advancing Translational Sciences)UL1 TR000445-06号基金的支持下进行。Precera Bioscience 公司为本研究提供了血清药物浓度测量结果。Eduard E. Vasilevskis 博士和 Sandra F. Simmons 博士得到了美国国立卫生研究院 R01AG53264 奖项的支持。Jin H. Han博士、Eduard E. Vasilevskis博士和Sandra F. Simmons博士还得到了退伍军人事务老年医学研究、教育和临床中心(GRECC)的支持。所有作者证明,他们与任何组织或实体均无关联,也未参与任何组织或实体的活动,这些组织或实体在本手稿所讨论的主题或材料中拥有任何经济利益或非经济利益。
Selective serotonin/serotonin-norepinephrine reuptake inhibitor serum concentrations' association with delirium duration
Delirium is a form of acute brain failure that commonly afflicts older hospitalized patients.1 The association between delirium and benzodiazepines is well-documented,2 but the association with other psychotropic medication classes is less clear. Using a novel liquid chromatography-mass spectrometry (LC-MS) assay, we observed supratherapeutic psychotropic drug levels (SPDLs) occurred in 17% of delirium cases and were associated with prolonged delirium episodes. Over half of SPDLs were secondary to selective and serotonin-norepinephrine reuptake inhibitors (SSRI/SNRIs),3 which are not considered deliriogenic.2 Most studies examining SSRI/SNRIs and delirium relied on medication lists, which do not account for SPDLs.4, 5 They also did not account for preexisting dementia, which may increase vulnerability to developing delirium, even at nontoxic, therapeutic drug concentrations.4, 5 We sought to determine if serum SSRI/SNRI concentrations were associated with prolonged delirium duration in older hospitalized adults and examined if this association was modified by preexisting dementia.
This was an exploratory analysis of a prospective cohort study.3, 6 Patients ≥65 years old who were admitted to the hospital, had serum available for LC-MS measurements, and enrolled within 4 h of emergency department presentation were included. All delirious and a random selection (~17%) of non-delirious patients were enrolled between March 2012 and November 2014.
Delirium was assessed daily using the modified Brief Confusion Assessment Method (bCAM), which is 82% sensitive and 96% specific for delirium.7 Serum SSRI/SNRI drug levels were measured using a LC-MS assay that measured 30+ psychotropic medications (Precera Bioscience, Inc., Franklin, TN). Standardized serum SSRI/SNRI concentrations were calculated by dividing each measurement by the upper limit of normal published in the literature. To establish the validity of our standardization approach, we analyzed standardized serum benzodiazepine concentrations. A patient was considered to have pre-illness dementia if they had: (i) a pre-illness dementia assessment (IQCODE) greater than 3.38,8 (ii) documented dementia diagnosis in the medical record, or (iii) prescribed cholinesterase inhibitors prior to admission.
To determine if standardized serum concentrations of SSRI/SNRIs or benzodiazepines were associated with delirium duration, proportional odds logistic regression was performed adjusting for age, pre-illness dementia, functional status, and depression, comorbidity burden, pre-illness severity, kidney/liver dysfunction, and central nervous system diagnosis.6 A standardized serum concentration*pre-illness dementia interaction was incorporated; effect modification was considered present if the p-value was <0.20. Adjusted odds ratios (aORs) with 95% confidence intervals (95% CI) are reported. Statistical analyses were performed on SAS version 9.3 (SAS Institute, Cary, NC).
Patient characteristics for the 158 patients included in this analysis can be seen in Supplemental Table 1. The median (interquartile range) delirium duration was 3 (2, 5) days. SSRI/SNRIs and benzodiazepines were detected in the sera in 54 (34.2%) and 26 (16.5%) patients, respectively. Of note, five out of 56 (8.9%) had SSRI/SNRIs and eight out of 26 (30.8%) had benzodiazepines detected by LC-MS, but were not listed in the electronic health record.
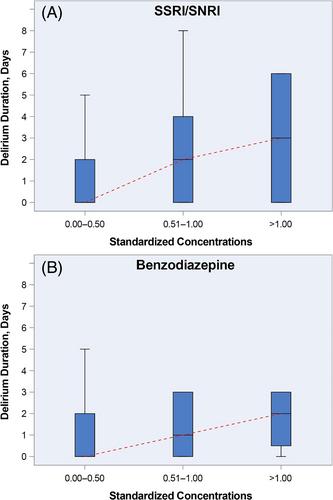
As standardized serum concentrations of SSRI/SNRI and benzodiazepines increased, delirium duration also increased (Figure 1). The aOR (95% CI) for the proportional odds logistic regression models evaluating the association between serum SSRI/SNRI and benzodiazepine concentrations and delirium duration are seen in Figure 2. In the adjusted analysis, standardized serum SSRI/SNRI concentrations were significantly associated with longer delirium duration in patients with preexisting dementia only (aOR = 2.4, 95% CI: 1.2, 4.7, p-value for interaction = 0.126). Standardized serum benzodiazepine concentrations were significantly associated with delirium duration, regardless of preexisting dementia status (aOR = 3.1, 95% CI: 1.1, 9.0, p-value for interaction = 0.265).
We observed that standardized serum SSRI/SNRI concentrations were associated with prolonged delirium duration in older hospitalized adults. The association was more prominent in those with preexisting dementia, who are the most vulnerable to developing delirium. This has multiple possible explanations: SSRI/SNRIs worsen delirium, may represent polypharmacy, serve as markers of advanced dementia with behavioral disturbances, or indicate aging physiology and reduced cognitive reserve. Further work is necessary to elucidate if SSRI/SNRIs have a causative effect on delirium duration. Most SSRI/SNRIs are not considered potentially inappropriate medications by established criteria.9 Our study suggests that older patients taking prescribed SSRI/SNRIs with delirium may benefit from serum concentration measurement. If elevated, dose reduction may be considered, especially if the patient has preexisting dementia. Because this was an exploratory analysis, our findings require confirmation.
We used a novel LC-MS assay to measure serum drug concentrations of psychotropic medications, which is a more accurate method to characterize drug exposure. Studies using medication lists can miss an average of two medications and do not take into account nonadherence.10 In our cohort, 9% and 31% of SSRI/SNRIs and benzodiazepines, respectively, were detected in the serum but were not documented in the electronic health record. LC-MS serum drug measurements can also account for toxic serum drug levels, which may lead to delirium and other adverse outcomes. This approach seems valid as standardized serum benzodiazepine concentrations were also associated with prolonged delirium.
Our study has several limitations. Residual confounding likely exists. We also did not evaluate the effect of SSRI/SNRIs on long-term cognition. A larger prospective cohort study is needed to examine this in older patients.
JHH designed the original DELINEATE study. JHH designed the exploratory analysis, supervised data collection, and performed the statistical analysis. JOJ, JHH had access to the entire data set. JHH performed the statistical analysis. JOJ, JHH wrote the primary manuscript draft. All authors provided substantial revisions and approved the final manuscript.
Dr. Jin H. Han and this study were funded by the National Institutes of Health under award number K23AG032355. This study was also supported by the National Center for Research Resources, Grant UL1 RR024975-01, and is now at the National Center for Advancing Translational Sciences, Grant 2 UL1 TR000445-06. Precera Bioscience, Inc, provided the serum drug concentration measurements for this study. Dr. Eduard E. Vasilevskis and Dr. Sandra F. Simmons are supported by the National Institutes of Health under award number R01AG53264. Dr. Jin H. Han, Dr. Eduard E. Vasilevskis, and Dr. Sandra F. Simmons are also supported by the Veteran Affairs Geriatric Research, Education, and Clinical Center (GRECC).
All authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this manuscript.
The sponsor had no role in the design of the study, the collection and analysis of the data, or the preparation of the manuscript.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
