Aleksei Baburin, Piret Veerus, Katrin Lang, Kaire Innos
{"title":"爱沙尼亚在引入有组织的乳房 X 射线照相筛查前后基于发病率的乳腺癌死亡率趋势:一项基于登记册的研究。","authors":"Aleksei Baburin, Piret Veerus, Katrin Lang, Kaire Innos","doi":"10.1177/10732748241266491","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite the relatively low breast cancer incidence in Estonia, mortality remains high, and participation in mammography screening is below the recommended 70%. The objective of this register-based study was to evaluate incidence-based (IB) breast cancer mortality before and after the introduction of organized mammography screening in 2004.</p><p><strong>Methods: </strong>Breast cancer deaths individually linked to breast cancer diagnosis were obtained from the Estonian Cancer Registry and used for calculating IB mortality. We compared age-specific IB mortality rates across 5-year birth cohorts and 5-year periods. Poisson regression was used to compare IB mortality for one age group invited to screening (50-63) and three age groups not invited to screening (30-49, 65-69, and 70+) during two periods before and after screening initiation (1993-2003 and 2004-2014). Joinpoint regression was used for age-standardized incidence and IB mortality trends.</p><p><strong>Results: </strong>Age-standardized IB mortality has been decreasing since 1997. Age-specific IB mortality for birth cohorts never exposed to screening showed a continuous increase with age, while in cohorts exposed to organized screening the mortality curve flattened or declined after the age of first invitation. Significant decreases in mortality from 1993-2003 to 2004-2014 were seen in the 30-49 (age-adjusted rate ratio 0.51, 95% CI 90.42-0.63) and 50-63 (0.65, 95% CI 0.56-0.74) age groups, while no decline was seen in the 65-69 and 70+ age groups.</p><p><strong>Conclusions: </strong>The age specific IB mortality curves in birth cohorts exposed to screening and the significant mortality decline in the target age group after the initiation of the organized program suggest a beneficial effect of screening. Improved treatment without screening has not reduced mortality in older age groups. Our results support raising the upper screening age limit to 74 years.</p>","PeriodicalId":49093,"journal":{"name":"Cancer Control","volume":"31 ","pages":"10732748241266491"},"PeriodicalIF":2.6000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11297520/pdf/","citationCount":"0","resultStr":"{\"title\":\"Incidence-Based Breast Cancer Mortality Trends in Estonia Before and After the Introduction of Organized Mammography Screening: A Register-Based Study.\",\"authors\":\"Aleksei Baburin, Piret Veerus, Katrin Lang, Kaire Innos\",\"doi\":\"10.1177/10732748241266491\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Despite the relatively low breast cancer incidence in Estonia, mortality remains high, and participation in mammography screening is below the recommended 70%. The objective of this register-based study was to evaluate incidence-based (IB) breast cancer mortality before and after the introduction of organized mammography screening in 2004.</p><p><strong>Methods: </strong>Breast cancer deaths individually linked to breast cancer diagnosis were obtained from the Estonian Cancer Registry and used for calculating IB mortality. We compared age-specific IB mortality rates across 5-year birth cohorts and 5-year periods. Poisson regression was used to compare IB mortality for one age group invited to screening (50-63) and three age groups not invited to screening (30-49, 65-69, and 70+) during two periods before and after screening initiation (1993-2003 and 2004-2014). Joinpoint regression was used for age-standardized incidence and IB mortality trends.</p><p><strong>Results: </strong>Age-standardized IB mortality has been decreasing since 1997. Age-specific IB mortality for birth cohorts never exposed to screening showed a continuous increase with age, while in cohorts exposed to organized screening the mortality curve flattened or declined after the age of first invitation. Significant decreases in mortality from 1993-2003 to 2004-2014 were seen in the 30-49 (age-adjusted rate ratio 0.51, 95% CI 90.42-0.63) and 50-63 (0.65, 95% CI 0.56-0.74) age groups, while no decline was seen in the 65-69 and 70+ age groups.</p><p><strong>Conclusions: </strong>The age specific IB mortality curves in birth cohorts exposed to screening and the significant mortality decline in the target age group after the initiation of the organized program suggest a beneficial effect of screening. Improved treatment without screening has not reduced mortality in older age groups. Our results support raising the upper screening age limit to 74 years.</p>\",\"PeriodicalId\":49093,\"journal\":{\"name\":\"Cancer Control\",\"volume\":\"31 \",\"pages\":\"10732748241266491\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11297520/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Control\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/10732748241266491\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Control","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/10732748241266491","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Incidence-Based Breast Cancer Mortality Trends in Estonia Before and After the Introduction of Organized Mammography Screening: A Register-Based Study.
Background: Despite the relatively low breast cancer incidence in Estonia, mortality remains high, and participation in mammography screening is below the recommended 70%. The objective of this register-based study was to evaluate incidence-based (IB) breast cancer mortality before and after the introduction of organized mammography screening in 2004.
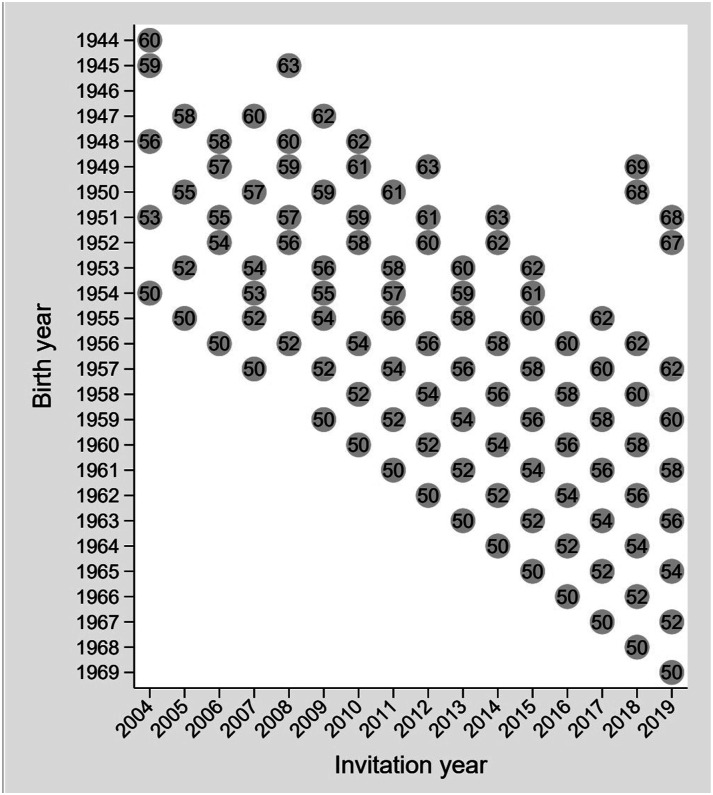
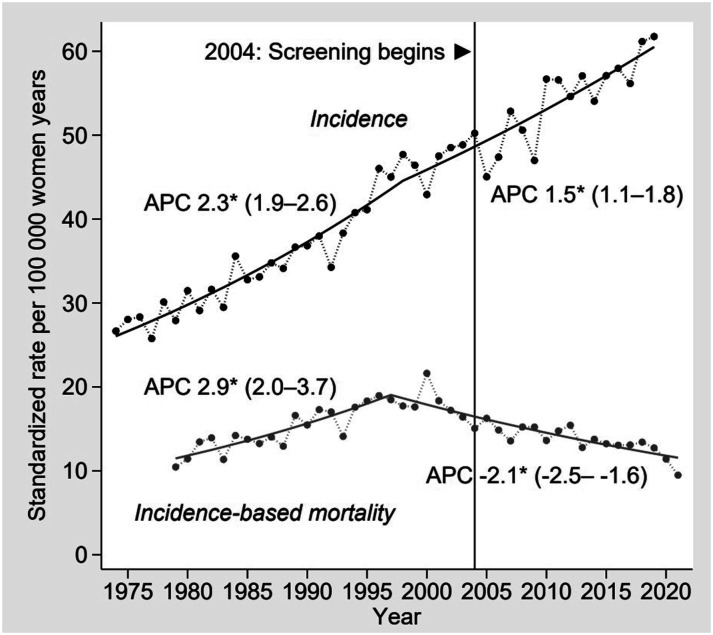
Methods: Breast cancer deaths individually linked to breast cancer diagnosis were obtained from the Estonian Cancer Registry and used for calculating IB mortality. We compared age-specific IB mortality rates across 5-year birth cohorts and 5-year periods. Poisson regression was used to compare IB mortality for one age group invited to screening (50-63) and three age groups not invited to screening (30-49, 65-69, and 70+) during two periods before and after screening initiation (1993-2003 and 2004-2014). Joinpoint regression was used for age-standardized incidence and IB mortality trends.
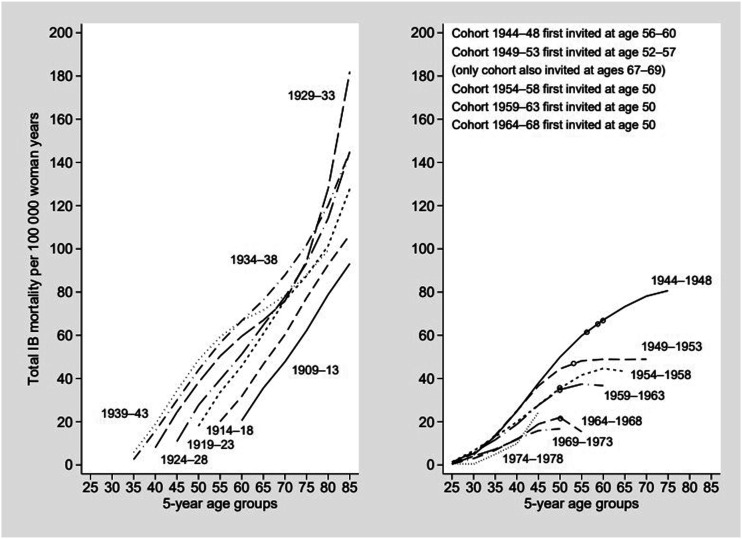
Results: Age-standardized IB mortality has been decreasing since 1997. Age-specific IB mortality for birth cohorts never exposed to screening showed a continuous increase with age, while in cohorts exposed to organized screening the mortality curve flattened or declined after the age of first invitation. Significant decreases in mortality from 1993-2003 to 2004-2014 were seen in the 30-49 (age-adjusted rate ratio 0.51, 95% CI 90.42-0.63) and 50-63 (0.65, 95% CI 0.56-0.74) age groups, while no decline was seen in the 65-69 and 70+ age groups.
Conclusions: The age specific IB mortality curves in birth cohorts exposed to screening and the significant mortality decline in the target age group after the initiation of the organized program suggest a beneficial effect of screening. Improved treatment without screening has not reduced mortality in older age groups. Our results support raising the upper screening age limit to 74 years.
期刊介绍:
Cancer Control is a JCR-ranked, peer-reviewed open access journal whose mission is to advance the prevention, detection, diagnosis, treatment, and palliative care of cancer by enabling researchers, doctors, policymakers, and other healthcare professionals to freely share research along the cancer control continuum. Our vision is a world where gold-standard cancer care is the norm, not the exception.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
