Yan Wang, Shilong Zhang, Bowen Ding, Zhaoqing Tang, Yuan Ji, Yiyi Yu, Yuehong Cui, Xuefei Wang, Yihong Sun, Tianshu Liu
{"title":"为接受根治术后围手术期化疗的胃癌患者制定并验证个体化提名图。","authors":"Yan Wang, Shilong Zhang, Bowen Ding, Zhaoqing Tang, Yuan Ji, Yiyi Yu, Yuehong Cui, Xuefei Wang, Yihong Sun, Tianshu Liu","doi":"10.21037/tgh-23-75","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prognostic factors are complicated and changeable for locally advanced gastric cancer (GC) patients. This study aimed to perform a novel prognostic model on survival for locally advanced GC patients who have received neoadjuvant chemotherapy and radical surgery.</p><p><strong>Methods: </strong>The locally advanced GC patients with neoadjuvant chemotherapy were included in this study from Zhongshan Hospital, Fudan University. A nomogram was developed based on independent prognostic factors identified through a multivariable Cox regression model. Model performance was evaluated in training and independent external cohorts in terms of calibration, discrimination, and clinical usefulness.</p><p><strong>Results: </strong>A total of 273 patients received radical resections. The median progression-free survival (PFS) and overall survival (OS) for all patients were 43.8 and 61.2 months, respectively. Nomogram showed that Lauren type made the greatest contribution to prognosis, followed by ypN. The prognostic nomogram had excellent discriminative ability, with a C-index of 0.689 [95% confidence interval (CI): 0.661-0.716], and an area under the receiver operating characteristic (ROC) curve (AUC) of 0.778, 0.746, and 0.725 for 3-, 5- and 10-year OS, respectively. Similar results were obtained in the external validation cohort. Based on the nomogram, the whole cohort was divided into high-risk and low-risk groups. And risk group classification was significantly associated with clinical characteristics, and produced an AUC value of 0.781, 0.748, and 0.727 for 3-, 5- and 10-year OS, respectively. Furthermore, compared with the tumor-node-metastasis (TNM) staging system (8th edition), Japanese criteria, and German criteria, the decision curve analysis (DCA) graphically demonstrated that the new model had more optimal net benefits in predicting the 3-, 5-, and 10-year OS for GC patients. Both C-index and time-dependent ROC curve demonstrated that the nomogram had a stronger capability for accurately predicting prognosis compared with the other staging system.</p><p><strong>Conclusions: </strong>The nomogram model is an effective support tool to predict OS in GC patients undergoing perioperative chemotherapy followed by radical surgery.</p>","PeriodicalId":94362,"journal":{"name":"Translational gastroenterology and hepatology","volume":"9 ","pages":"39"},"PeriodicalIF":2.5000,"publicationDate":"2024-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11292059/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development and validation of an individualized nomogram for gastric cancer patients treated with perioperative chemotherapy followed by radical surgery.\",\"authors\":\"Yan Wang, Shilong Zhang, Bowen Ding, Zhaoqing Tang, Yuan Ji, Yiyi Yu, Yuehong Cui, Xuefei Wang, Yihong Sun, Tianshu Liu\",\"doi\":\"10.21037/tgh-23-75\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Prognostic factors are complicated and changeable for locally advanced gastric cancer (GC) patients. This study aimed to perform a novel prognostic model on survival for locally advanced GC patients who have received neoadjuvant chemotherapy and radical surgery.</p><p><strong>Methods: </strong>The locally advanced GC patients with neoadjuvant chemotherapy were included in this study from Zhongshan Hospital, Fudan University. A nomogram was developed based on independent prognostic factors identified through a multivariable Cox regression model. Model performance was evaluated in training and independent external cohorts in terms of calibration, discrimination, and clinical usefulness.</p><p><strong>Results: </strong>A total of 273 patients received radical resections. The median progression-free survival (PFS) and overall survival (OS) for all patients were 43.8 and 61.2 months, respectively. Nomogram showed that Lauren type made the greatest contribution to prognosis, followed by ypN. The prognostic nomogram had excellent discriminative ability, with a C-index of 0.689 [95% confidence interval (CI): 0.661-0.716], and an area under the receiver operating characteristic (ROC) curve (AUC) of 0.778, 0.746, and 0.725 for 3-, 5- and 10-year OS, respectively. Similar results were obtained in the external validation cohort. Based on the nomogram, the whole cohort was divided into high-risk and low-risk groups. And risk group classification was significantly associated with clinical characteristics, and produced an AUC value of 0.781, 0.748, and 0.727 for 3-, 5- and 10-year OS, respectively. Furthermore, compared with the tumor-node-metastasis (TNM) staging system (8th edition), Japanese criteria, and German criteria, the decision curve analysis (DCA) graphically demonstrated that the new model had more optimal net benefits in predicting the 3-, 5-, and 10-year OS for GC patients. Both C-index and time-dependent ROC curve demonstrated that the nomogram had a stronger capability for accurately predicting prognosis compared with the other staging system.</p><p><strong>Conclusions: </strong>The nomogram model is an effective support tool to predict OS in GC patients undergoing perioperative chemotherapy followed by radical surgery.</p>\",\"PeriodicalId\":94362,\"journal\":{\"name\":\"Translational gastroenterology and hepatology\",\"volume\":\"9 \",\"pages\":\"39\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-06-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11292059/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational gastroenterology and hepatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/tgh-23-75\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/tgh-23-75","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:局部晚期胃癌(GC)患者的预后因素复杂多变:局部晚期胃癌(GC)患者的预后因素复杂多变。本研究旨在为接受新辅助化疗和根治性手术的局部晚期胃癌患者建立一个新的生存预后模型:方法:本研究纳入了复旦大学附属中山医院接受新辅助化疗的局部晚期胃癌患者。根据多变量 Cox 回归模型确定的独立预后因素建立了一个提名图。在训练队列和独立外部队列中对模型的校准、区分度和临床实用性进行了评估:共有 273 名患者接受了根治性切除术。所有患者的中位无进展生存期(PFS)和总生存期(OS)分别为43.8个月和61.2个月。预后提名图显示,劳伦型对预后的影响最大,其次是ypN。预后提名图具有很好的鉴别能力,C指数为0.689[95%置信区间(CI):0.661-0.716],3年、5年和10年OS的接收器操作特征曲线下面积(AUC)分别为0.778、0.746和0.725。外部验证队列也得到了类似的结果。根据提名图,整个队列被分为高风险组和低风险组。而风险组的划分与临床特征有明显相关性,3年、5年和10年OS的AUC值分别为0.781、0.748和0.727。此外,与肿瘤-结节-转移(TNM)分期系统(第 8 版)、日本标准和德国标准相比,决策曲线分析(DCA)以图形方式表明,新模型在预测 GC 患者 3 年、5 年和 10 年 OS 方面具有更理想的净效益。C指数和随时间变化的ROC曲线都表明,与其他分期系统相比,提名图具有更强的准确预测预后的能力:结论:提名图模型是预测接受根治术后围手术期化疗的 GC 患者 OS 的有效辅助工具。
Development and validation of an individualized nomogram for gastric cancer patients treated with perioperative chemotherapy followed by radical surgery.
Background: Prognostic factors are complicated and changeable for locally advanced gastric cancer (GC) patients. This study aimed to perform a novel prognostic model on survival for locally advanced GC patients who have received neoadjuvant chemotherapy and radical surgery.
Methods: The locally advanced GC patients with neoadjuvant chemotherapy were included in this study from Zhongshan Hospital, Fudan University. A nomogram was developed based on independent prognostic factors identified through a multivariable Cox regression model. Model performance was evaluated in training and independent external cohorts in terms of calibration, discrimination, and clinical usefulness.
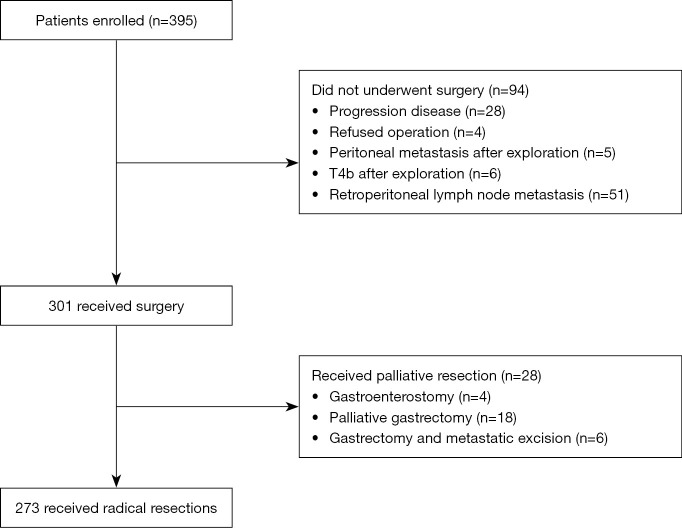
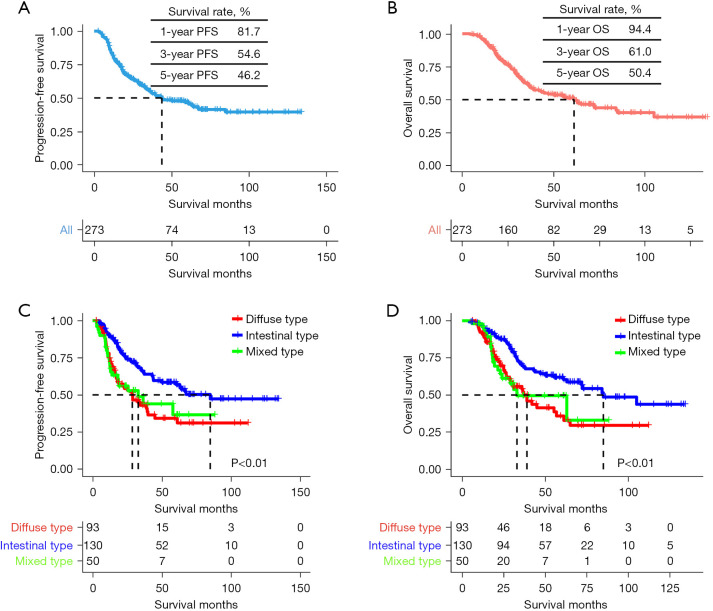
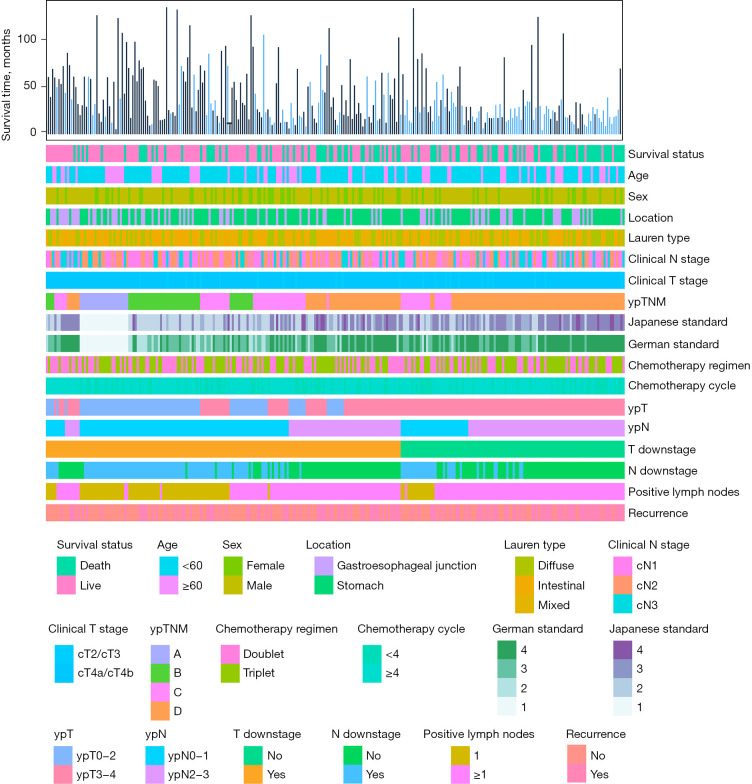
Results: A total of 273 patients received radical resections. The median progression-free survival (PFS) and overall survival (OS) for all patients were 43.8 and 61.2 months, respectively. Nomogram showed that Lauren type made the greatest contribution to prognosis, followed by ypN. The prognostic nomogram had excellent discriminative ability, with a C-index of 0.689 [95% confidence interval (CI): 0.661-0.716], and an area under the receiver operating characteristic (ROC) curve (AUC) of 0.778, 0.746, and 0.725 for 3-, 5- and 10-year OS, respectively. Similar results were obtained in the external validation cohort. Based on the nomogram, the whole cohort was divided into high-risk and low-risk groups. And risk group classification was significantly associated with clinical characteristics, and produced an AUC value of 0.781, 0.748, and 0.727 for 3-, 5- and 10-year OS, respectively. Furthermore, compared with the tumor-node-metastasis (TNM) staging system (8th edition), Japanese criteria, and German criteria, the decision curve analysis (DCA) graphically demonstrated that the new model had more optimal net benefits in predicting the 3-, 5-, and 10-year OS for GC patients. Both C-index and time-dependent ROC curve demonstrated that the nomogram had a stronger capability for accurately predicting prognosis compared with the other staging system.
Conclusions: The nomogram model is an effective support tool to predict OS in GC patients undergoing perioperative chemotherapy followed by radical surgery.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
