Sean J. Barbour , Rosanna Coppo , Lee Er , Maria Luisa Russo , Zhi-Hong Liu , Jie Ding , Xuhui Zhong , Ritsuko Katafuchi , Norishige Yoshikawa , Hong Xu , Shoji Kagami , Yukio Yuzawa , Francesco Emma , Alexandra Cambier , Licia Peruzzi , Robert J. Wyatt , Daniel C. Cattran
{"title":"在活组织切片检查后一两年的儿童中应用最新的国际 IgA 肾病预测工具。","authors":"Sean J. Barbour , Rosanna Coppo , Lee Er , Maria Luisa Russo , Zhi-Hong Liu , Jie Ding , Xuhui Zhong , Ritsuko Katafuchi , Norishige Yoshikawa , Hong Xu , Shoji Kagami , Yukio Yuzawa , Francesco Emma , Alexandra Cambier , Licia Peruzzi , Robert J. Wyatt , Daniel C. Cattran","doi":"10.1016/j.kint.2024.07.012","DOIUrl":null,"url":null,"abstract":"<div><div>The pediatric International IgA Nephropathy (IgAN) Prediction Tool comprises two models with and without ethnicity and is the first method to predict the risk of a 30% decline in estimated glomerular filtration rate (eGFR) or kidney failure in children at the time of biopsy using clinical risk factors and Oxford MEST histology scores. However, it is unknown if the Prediction Tool can be applied after a period of observation post-biopsy. Using an international multi-ethnic cohort of 947 children with IgAN, 38% of whom were followed into adulthood, the Prediction Tool was updated for use one year after biopsy. Compared to the original pediatric Prediction Tool, the updated post-biopsy Prediction Tool had a better model fit with higher R<sup>2</sup><sub>D</sub> (51%/50% vs 20%), significant increase in 4-year C-statistics (0.83 vs 0.73/0.69, ΔC 0.09 [95% confidence interval 0.07-0.10] and ΔC 0.14 [0.12-0.15]) and better 4-year calibration with lower integrated calibration indices (0.74/0.54 vs 2.45/1.01). Results were similar after internal validation and when the models were applied two years after biopsy. Trajectories of eGFR after a baseline one year post-biopsy were non-linear and those at higher predicted risk started with a lower eGFR and experienced a more rapid decline over time. In children, eGFR had a variable rate of increase until 15-18 years old and then decreased linearly with a more rapid decline in higher risk groups that was similar to young adults of comparable risk. Thus, the original pediatric Prediction Tool should be used in children at the time of biopsy, and the updated pediatric Prediction Tool should be used to re-evaluate risk one or two years after biopsy.</div></div>","PeriodicalId":17801,"journal":{"name":"Kidney international","volume":"106 5","pages":"Pages 913-927"},"PeriodicalIF":21.8000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Application of the updated International IgA Nephropathy Prediction Tool in children one or two years post-biopsy\",\"authors\":\"Sean J. Barbour , Rosanna Coppo , Lee Er , Maria Luisa Russo , Zhi-Hong Liu , Jie Ding , Xuhui Zhong , Ritsuko Katafuchi , Norishige Yoshikawa , Hong Xu , Shoji Kagami , Yukio Yuzawa , Francesco Emma , Alexandra Cambier , Licia Peruzzi , Robert J. Wyatt , Daniel C. Cattran\",\"doi\":\"10.1016/j.kint.2024.07.012\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><div>The pediatric International IgA Nephropathy (IgAN) Prediction Tool comprises two models with and without ethnicity and is the first method to predict the risk of a 30% decline in estimated glomerular filtration rate (eGFR) or kidney failure in children at the time of biopsy using clinical risk factors and Oxford MEST histology scores. However, it is unknown if the Prediction Tool can be applied after a period of observation post-biopsy. Using an international multi-ethnic cohort of 947 children with IgAN, 38% of whom were followed into adulthood, the Prediction Tool was updated for use one year after biopsy. Compared to the original pediatric Prediction Tool, the updated post-biopsy Prediction Tool had a better model fit with higher R<sup>2</sup><sub>D</sub> (51%/50% vs 20%), significant increase in 4-year C-statistics (0.83 vs 0.73/0.69, ΔC 0.09 [95% confidence interval 0.07-0.10] and ΔC 0.14 [0.12-0.15]) and better 4-year calibration with lower integrated calibration indices (0.74/0.54 vs 2.45/1.01). Results were similar after internal validation and when the models were applied two years after biopsy. Trajectories of eGFR after a baseline one year post-biopsy were non-linear and those at higher predicted risk started with a lower eGFR and experienced a more rapid decline over time. In children, eGFR had a variable rate of increase until 15-18 years old and then decreased linearly with a more rapid decline in higher risk groups that was similar to young adults of comparable risk. Thus, the original pediatric Prediction Tool should be used in children at the time of biopsy, and the updated pediatric Prediction Tool should be used to re-evaluate risk one or two years after biopsy.</div></div>\",\"PeriodicalId\":17801,\"journal\":{\"name\":\"Kidney international\",\"volume\":\"106 5\",\"pages\":\"Pages 913-927\"},\"PeriodicalIF\":21.8000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Kidney international\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0085253824005325\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney international","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0085253824005325","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/31 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
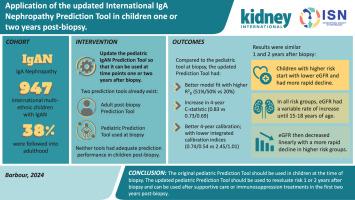
儿科国际 IgA 肾病(IgAN)预测工具包括两个模型,分别包含种族因素和不包含种族因素,是首个利用临床风险因素和牛津 MEST 组织学评分预测儿童活检时估计肾小球滤过率(eGFR)下降 30% 或肾衰竭风险的方法。然而,预测工具能否在活检后的观察期后应用尚不得而知。我们利用一个由947名IgAN患儿组成的多种族国际队列,对预测工具进行了更新,以便在活检一年后使用。与最初的儿科预测工具相比,活检后更新的预测工具具有更好的模型拟合度,R2D更高(51%/50% vs 20%),4年C统计量显著增加(0.83 vs 0.73/0.69, ΔC 0.09 [95%置信区间0.07-0.10]和ΔC 0.14 [0.12-0.15]),4年校准效果更好,综合校准指数更低(0.74/0.54 vs 2.45/1.01)。内部验证和活检两年后应用模型的结果相似。活组织检查后一年的 eGFR 基线轨迹是非线性的,预测风险较高的人开始时 eGFR 较低,随着时间的推移下降得更快。在儿童中,eGFR 在 15-18 岁之前的增长速度不一,之后呈线性下降,高风险组的下降速度更快,这与风险相当的年轻成人相似。因此,原始的儿科预测工具应在活检时用于儿童,而更新的儿科预测工具则应在活检后一两年用于重新评估风险。
Application of the updated International IgA Nephropathy Prediction Tool in children one or two years post-biopsy
The pediatric International IgA Nephropathy (IgAN) Prediction Tool comprises two models with and without ethnicity and is the first method to predict the risk of a 30% decline in estimated glomerular filtration rate (eGFR) or kidney failure in children at the time of biopsy using clinical risk factors and Oxford MEST histology scores. However, it is unknown if the Prediction Tool can be applied after a period of observation post-biopsy. Using an international multi-ethnic cohort of 947 children with IgAN, 38% of whom were followed into adulthood, the Prediction Tool was updated for use one year after biopsy. Compared to the original pediatric Prediction Tool, the updated post-biopsy Prediction Tool had a better model fit with higher R2D (51%/50% vs 20%), significant increase in 4-year C-statistics (0.83 vs 0.73/0.69, ΔC 0.09 [95% confidence interval 0.07-0.10] and ΔC 0.14 [0.12-0.15]) and better 4-year calibration with lower integrated calibration indices (0.74/0.54 vs 2.45/1.01). Results were similar after internal validation and when the models were applied two years after biopsy. Trajectories of eGFR after a baseline one year post-biopsy were non-linear and those at higher predicted risk started with a lower eGFR and experienced a more rapid decline over time. In children, eGFR had a variable rate of increase until 15-18 years old and then decreased linearly with a more rapid decline in higher risk groups that was similar to young adults of comparable risk. Thus, the original pediatric Prediction Tool should be used in children at the time of biopsy, and the updated pediatric Prediction Tool should be used to re-evaluate risk one or two years after biopsy.
期刊介绍:
Kidney International (KI), the official journal of the International Society of Nephrology, is led by Dr. Pierre Ronco (Paris, France) and stands as one of nephrology's most cited and esteemed publications worldwide.
KI provides exceptional benefits for both readers and authors, featuring highly cited original articles, focused reviews, cutting-edge imaging techniques, and lively discussions on controversial topics.
The journal is dedicated to kidney research, serving researchers, clinical investigators, and practicing nephrologists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
