Samer Al Hadidi, Obada Ababneh, Carolina Schinke, Sharmilan Thanendrarajan, Clyde Bailey, Guido Tricot, John Shaughnessy Jr, Fenghuang Zhan, Jeffrey Sawyer, Eric R. Siegel, Maurizio Zangari, Bart Barlogie, Frits van Rhee
{"title":"多发性骨髓瘤串联自体造血干细胞移植后的第二原发性恶性肿瘤。","authors":"Samer Al Hadidi, Obada Ababneh, Carolina Schinke, Sharmilan Thanendrarajan, Clyde Bailey, Guido Tricot, John Shaughnessy Jr, Fenghuang Zhan, Jeffrey Sawyer, Eric R. Siegel, Maurizio Zangari, Bart Barlogie, Frits van Rhee","doi":"10.1002/ajh.27452","DOIUrl":null,"url":null,"abstract":"<p>Autologous hematopoietic stem cell transplantation (HSCT) is a standard treatment for eligible multiple myeloma (MM) patients.<span><sup>1</sup></span> Before high-dose chemotherapy and autologous HSCT, patients typically receive induction therapy with a proteasome inhibitor and an immunomodulatory (IMiD) agent. This approach, along with posttransplant maintenance therapies, has improved survival, with some patients achieving a median overall survival (OS) of over 10 years.<span><sup>1</sup></span></p><p>While late mortality rates have decreased over the past three decades, the incidence of second primary malignancies (SPM) has not.<span><sup>2</sup></span> Given improved survival rates, understanding long-term complications like SPM is crucial, particularly as most phase III MM trials lack extended follow-up.<span><sup>3</sup></span></p><p>Autologous HSCT enhances long-term disease control and survival in newly diagnosed MM patients but increases the risk of SPM, including second hematologic malignancies (SHM). A Swedish study found that higher cumulative doses of melphalan were linked to a 2.8-fold increased risk of therapy-related myeloid neoplasms.<span><sup>4</sup></span> In a study of 3948 MM patients, 4% developed SPM, with 64% being solid tumors, 20% myeloid, 14% SHM, and 2% lymphoid malignancies. This study included only single autologous HSCT patients and had a median follow-up of 37 months, limiting the assessment of late SPM development.<span><sup>5</sup></span></p><p>The principal objective of this study was to examine the occurrence and attributes of SPM and their subsequent effects on OS. Additionally, we sought to investigate whether the utilization of tandem autologous HSCT was associated with an elevated risk of SPM in comparison with single autologous HSCT. Secondary aims included the classification of various SPM types that emerged following autologous HSCT. Methods are detailed in supplementary.</p><p>A total of 1379 patients with newly diagnosed MM enrolled on four TT trials. An overview of the patients' characteristics can be found in [Table S1]. The median follow-up durations varied across different treatment groups: 25.3 years for TT I, 20.4 years for TT II (Arm A), 19.8 years for TT II (Arm B), 17.1 years for TT IIIA, and 15.4 years for TT IIIB. When considering the entire cohort of 1379 patients in the study, the median follow-up period was 16.6 years, with an interquartile range (IQR) spanning from 13.5 to 20 years. A total of 2640 transplants were performed on patients in our study cohort, with most of the transplants as first autologous HSCT (<i>n</i> = 1267) and second autologous HSCT (<i>n</i> = 1034) [Table S2]. Patients' baseline characteristics according to the type of transplant are summarized in [Table S3]. Overall, among the total of 1379 enrolled patients in the study, 974 patients (71%) underwent tandem autologous HSCT, with an average time interval of approximately 3.2 months between the first and second autologous HSCT [Table S4]. Event rates of SPM, characteristics of patients with more than one SPM, and survival analysis based on SPM are summarized in Supplementary (Figure S1–S6 and Table S5).</p><p>A total of 78 (5.6%) patients were diagnosed with any SHM. Myelodysplastic syndrome (MDS) alone, MDS with myeloproliferative neoplasms (MDS/MPN) and acute myelogenous leukemia (AML) occurred in 61 (4.4%) of patients. Acute lymphoblastic leukemia (ALL) occurred only in four (0.3%) of patients. A fitted Poisson regression was used to determine the event rate of SHM and the statistical differences between trials. There was a significant difference of SHM event rates between trials (TT I = 3.9/kPY; 95%CI: 2–7.8, TT II (Arm A) = 5.3/kPY; 95%CI: 3.3–8.6, TT II (Arm B) = 6.9/kPY; 95%CI: 4.5–10.6, TT IIIA = 9.3/kPY; 95%CI: 6.4–13.6, TT IIIB = 3.3/kPY; 95%CI: 1.4–7.9, <i>p</i> < .001). Based on pairwise comparisons, SHM event rates in TT I were similar compared with TT II (Arm A) (IRR = 0.44, <i>p</i> = .044), TT II (Arm B) (IRR = 0.61, <i>p</i> = .28), TT IIIA (IRR = 0.38, <i>p</i> = .017), and TT IIIB (IRR = 1.15, <i>p</i> = .77). TT IIIA SHM rate was similar to TT IIIB (IRR = 1.51, <i>p</i> = .29). Other event rates did not differ between trials (<i>p</i> > .01 for pairwise comparisons). The percentage of tandem autologous HSCT was higher in TT IIIA (85%) and TT IIIB (84%) when compared with TT I (59%), TT II (arm A) (65%) and TT II (Arm B) (65%) (chi-square <i>p</i> < .001). In addition, the event rate of SHM in patients who received tandem autologous HSCT was similar the only one transplant (IRR = 1.02, <i>p</i> = .99). It was also similar when comparing tandem with non-tandem double transplant (IRR = 0.47, <i>p</i> = .06). Based on a specific SHM type, no statistical difference was found between protocols. Details of SHM according to protocol are summarized in Table.S6.</p><p>At a median follow-up period of 15 years, the majority of surviving patients did not exhibit SHM. The proportion of patients with SHM at 15 years was as follows: 7.4% in the TT I group (95% CI: 1.3–13.1%), 6.4% in the TT II (arm A) group (95% CI: 2.5–10.1%), 8% in the TT II (arm B) group (95% CI: 3.6–12.1%), 8% in the TT IIIA group (95% CI: 4.2–11.6%), and 3.8% in the TT IIIB group (95% CI: 0–3.4%). Figure 1. RMTL analysis did not find a statistical difference between TT IIIA versus TT IIIB (<i>p</i> = .246) and tandem versus single transplant (<i>p</i> = .767).</p><p>Secondary solid cancers were observed in 7.6% of the study cohort, encompassing 105 cases out of a total of 1379 patients. Eight patients had more than one solid malignancy. The most prevalent secondary solid cancers were prostate cancer (22 tumors), breast cancer (15 tumors), and colorectal cancer (15 tumors). There was no significant difference of secondary solid cancers event rates between trials (TT I = 5.72/kPY; 95%CI: 3.25–10.08, TT II (arm A) = 10.62/kPY; 95%CI: 7.62–14.79, TT II (arm B) = 9.5/kPY; 95%CI: 6.64–13.59, TT IIIA = 5.35/kPY; 95%CI: 3.28–8.73, TT IIIB = 7.87/kPY; 95%CI: 4.47–13.87, <i>p</i> = .6). The event rate of secondary solid cancers in patients who received tandem autologous HSCT was similar the only one transplant (IRR = 1.1, <i>p</i> = .8). Similarly, there was no difference in secondary solid cancers event rates between tandem and non-tandem double transplant (IRR = 0.88, <i>p</i> = .75). Details of secondary solid cancers according to protocol are summarized in Table S7.</p><p>At the 15-year median follow-up point, it was observed that the majority of surviving patients did not develop solid malignancies. The proportion of patients with secondary solid cancers at 15 years was as follows: 8.5% in TT I (95% CI: 1.6–14.8%), 15.7% in TT II (arm A) (95% CI: 11.1–20%), 13.6% in TT II (arm B) (95% CI: 9.8–18%), 8.2% in TT IIIA (95% CI: 3.7–12.5%), and 10.9% in TT IIIB (95% CI: 3.4–16%). Figure S7.</p><p>To our knowledge, this is the largest and most comprehensive analysis with the longest follow-up duration to report on risk of SPM in MM patients who underwent tandem autologous HSCT. The incidence of SHM and secondary solid malignancies in patients undergoing tandem autologous HSCT on earlier TT protocols, with a median follow-up exceeding 15 years, was relatively low at 6.8% and 8.6%, respectively. Our extended follow-up revealed a relatively low risk of developing MDS and/or AML and/or MDS/MPN of 4.4%.</p><p>The International Myeloma Working Group (IMWG) suggests an intensified monitoring approach and precise quantification of second cancers in the context of clinical trials, proposing the inclusion of SPM as a defined endpoint. With the improvement of OS, patients need to undergo age-appropriate cancer screening. Our study revealed that the most common secondary solid malignancies were prostate cancer, breast cancer, and colon cancer. Such cancers are common and there are various guidelines that support screening of the general population for early detection and/or intervention.</p><p>The emergence of SHM or secondary solid malignancy was correlated with worse OS. This underscores the importance of vigilance in monitoring and managing these complications. Our findings emphasize that autologous transplantation in MM, particularly tandem autologous transplant in our trials, led to a significant improvement in OS even before the era of anti-CD38 monoclonal antibodies, bispecific antibodies, and chimeric antigen T-cell receptor therapy. This implies that early consideration of autotransplant, especially in eligible patients, can positively influence long-term outcomes. Our analysis revealed no difference in the risk of SHM between patients undergoing single versus tandem autologous HSCT. The risk is relatively low for both types (5.6%) even with long follow-up duration (16.6 years). While tandem autologous HSCT is used less frequently nowadays, it is still considered as standard of care in high-risk MM per the European Hematology Association (EHA)-European Society for Medical Oncology (ESMO) Clinical Practice Guidelines. The National Comprehensive Cancer Network (NCCN) guidelines suggest that tandem autologous HSCT can be considered for all patients who are candidates for transplant and is an option for patients who done not achieve at least a very good partial response after first autologous HSCT and in high-risk MM. It is our practice to offer tandem autologous HSCT in young patients and patients with high-risk disease.<span><sup>6</sup></span></p><p>Clonal hematopoiesis of indeterminate potential (CHIP) is associated with a small risk of progression to MDS and/or AML. Its prevalence is higher in older populations and in patients who received chemotherapy.<span><sup>7</sup></span> Unfortunately, CHIP data are not available for our patients, so we cannot determine if the MDS and AML cases were a consequence of CHIP. In addition, CHIP was associated with poor OS and PFS in patients receiving HSCT for MM.<span><sup>8</sup></span></p><p>Tandem autologous HSCT was not associated with increased risk of SHM when compared with single autologous HSCT (6.8% vs. 4.3%) and no statistically significant difference in secondary solid malignancies (8.6% vs. 5.6%). Median OS was longer in patients who underwent tandem autologous HSCT: 10.88 years (95% CI: 9.85–11.74 years) compared with 6.08 years (95% CI: 4.58–7.74 years), <i>p</i>-value <.001. Although the tandem approach did not increase the rate of malignancies, we emphasize the need for rigorous screening in older MM patients, with specific recommendations for monitoring hematologic abnormalities and common solid tumors like breast, prostate, colorectal cancer, and melanoma according to established guidelines. Patients included were not treated with upfront novel agents such as anti-CD38 monoclonal antibodies, bispecific antibodies, or Chimeric Antigen Receptor T-cell (CAR T) cells, which have significantly changed the treatment landscape. Future trials will report on the risk of secondary malignancies associated with these new approaches.</p><p>In conclusion, our study comprehensively examines SPM in MM patients treated with autologous HSCT under various earlier TT protocols. The occurrence of SHM and secondary solid malignancies in patients treated with tandem autologous HSCT on earlier TT protocols and followed for a median of over 15 years was relatively low. Autologous HSCT in MM, particularly tandem autologous HSCT in our trials, significantly improved OS and should be offered early to eligible patients.</p><p><b>Conceived and designed the analysis:</b> SAH, CS, GT, ERS, BB, FVR. <b>Performed and assisted analysis:</b> SAH, OA, and E.RS. <b>Wrote the original draft of the paper:</b> SAH. <b>Reviewed and edited the paper:</b> All authors.</p><p>SAH reports receiving consulting fees from Jansen, Pfizer, and Sanofi.</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"99 11","pages":"2222-2224"},"PeriodicalIF":9.9000,"publicationDate":"2024-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27452","citationCount":"0","resultStr":"{\"title\":\"Second primary malignancies after tandem autologous hematopoietic stem cell transplantation for multiple myeloma\",\"authors\":\"Samer Al Hadidi, Obada Ababneh, Carolina Schinke, Sharmilan Thanendrarajan, Clyde Bailey, Guido Tricot, John Shaughnessy Jr, Fenghuang Zhan, Jeffrey Sawyer, Eric R. Siegel, Maurizio Zangari, Bart Barlogie, Frits van Rhee\",\"doi\":\"10.1002/ajh.27452\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Autologous hematopoietic stem cell transplantation (HSCT) is a standard treatment for eligible multiple myeloma (MM) patients.<span><sup>1</sup></span> Before high-dose chemotherapy and autologous HSCT, patients typically receive induction therapy with a proteasome inhibitor and an immunomodulatory (IMiD) agent. This approach, along with posttransplant maintenance therapies, has improved survival, with some patients achieving a median overall survival (OS) of over 10 years.<span><sup>1</sup></span></p><p>While late mortality rates have decreased over the past three decades, the incidence of second primary malignancies (SPM) has not.<span><sup>2</sup></span> Given improved survival rates, understanding long-term complications like SPM is crucial, particularly as most phase III MM trials lack extended follow-up.<span><sup>3</sup></span></p><p>Autologous HSCT enhances long-term disease control and survival in newly diagnosed MM patients but increases the risk of SPM, including second hematologic malignancies (SHM). A Swedish study found that higher cumulative doses of melphalan were linked to a 2.8-fold increased risk of therapy-related myeloid neoplasms.<span><sup>4</sup></span> In a study of 3948 MM patients, 4% developed SPM, with 64% being solid tumors, 20% myeloid, 14% SHM, and 2% lymphoid malignancies. This study included only single autologous HSCT patients and had a median follow-up of 37 months, limiting the assessment of late SPM development.<span><sup>5</sup></span></p><p>The principal objective of this study was to examine the occurrence and attributes of SPM and their subsequent effects on OS. Additionally, we sought to investigate whether the utilization of tandem autologous HSCT was associated with an elevated risk of SPM in comparison with single autologous HSCT. Secondary aims included the classification of various SPM types that emerged following autologous HSCT. Methods are detailed in supplementary.</p><p>A total of 1379 patients with newly diagnosed MM enrolled on four TT trials. An overview of the patients' characteristics can be found in [Table S1]. The median follow-up durations varied across different treatment groups: 25.3 years for TT I, 20.4 years for TT II (Arm A), 19.8 years for TT II (Arm B), 17.1 years for TT IIIA, and 15.4 years for TT IIIB. When considering the entire cohort of 1379 patients in the study, the median follow-up period was 16.6 years, with an interquartile range (IQR) spanning from 13.5 to 20 years. A total of 2640 transplants were performed on patients in our study cohort, with most of the transplants as first autologous HSCT (<i>n</i> = 1267) and second autologous HSCT (<i>n</i> = 1034) [Table S2]. Patients' baseline characteristics according to the type of transplant are summarized in [Table S3]. Overall, among the total of 1379 enrolled patients in the study, 974 patients (71%) underwent tandem autologous HSCT, with an average time interval of approximately 3.2 months between the first and second autologous HSCT [Table S4]. Event rates of SPM, characteristics of patients with more than one SPM, and survival analysis based on SPM are summarized in Supplementary (Figure S1–S6 and Table S5).</p><p>A total of 78 (5.6%) patients were diagnosed with any SHM. Myelodysplastic syndrome (MDS) alone, MDS with myeloproliferative neoplasms (MDS/MPN) and acute myelogenous leukemia (AML) occurred in 61 (4.4%) of patients. Acute lymphoblastic leukemia (ALL) occurred only in four (0.3%) of patients. A fitted Poisson regression was used to determine the event rate of SHM and the statistical differences between trials. There was a significant difference of SHM event rates between trials (TT I = 3.9/kPY; 95%CI: 2–7.8, TT II (Arm A) = 5.3/kPY; 95%CI: 3.3–8.6, TT II (Arm B) = 6.9/kPY; 95%CI: 4.5–10.6, TT IIIA = 9.3/kPY; 95%CI: 6.4–13.6, TT IIIB = 3.3/kPY; 95%CI: 1.4–7.9, <i>p</i> < .001). Based on pairwise comparisons, SHM event rates in TT I were similar compared with TT II (Arm A) (IRR = 0.44, <i>p</i> = .044), TT II (Arm B) (IRR = 0.61, <i>p</i> = .28), TT IIIA (IRR = 0.38, <i>p</i> = .017), and TT IIIB (IRR = 1.15, <i>p</i> = .77). TT IIIA SHM rate was similar to TT IIIB (IRR = 1.51, <i>p</i> = .29). Other event rates did not differ between trials (<i>p</i> > .01 for pairwise comparisons). The percentage of tandem autologous HSCT was higher in TT IIIA (85%) and TT IIIB (84%) when compared with TT I (59%), TT II (arm A) (65%) and TT II (Arm B) (65%) (chi-square <i>p</i> < .001). In addition, the event rate of SHM in patients who received tandem autologous HSCT was similar the only one transplant (IRR = 1.02, <i>p</i> = .99). It was also similar when comparing tandem with non-tandem double transplant (IRR = 0.47, <i>p</i> = .06). Based on a specific SHM type, no statistical difference was found between protocols. Details of SHM according to protocol are summarized in Table.S6.</p><p>At a median follow-up period of 15 years, the majority of surviving patients did not exhibit SHM. The proportion of patients with SHM at 15 years was as follows: 7.4% in the TT I group (95% CI: 1.3–13.1%), 6.4% in the TT II (arm A) group (95% CI: 2.5–10.1%), 8% in the TT II (arm B) group (95% CI: 3.6–12.1%), 8% in the TT IIIA group (95% CI: 4.2–11.6%), and 3.8% in the TT IIIB group (95% CI: 0–3.4%). Figure 1. RMTL analysis did not find a statistical difference between TT IIIA versus TT IIIB (<i>p</i> = .246) and tandem versus single transplant (<i>p</i> = .767).</p><p>Secondary solid cancers were observed in 7.6% of the study cohort, encompassing 105 cases out of a total of 1379 patients. Eight patients had more than one solid malignancy. The most prevalent secondary solid cancers were prostate cancer (22 tumors), breast cancer (15 tumors), and colorectal cancer (15 tumors). There was no significant difference of secondary solid cancers event rates between trials (TT I = 5.72/kPY; 95%CI: 3.25–10.08, TT II (arm A) = 10.62/kPY; 95%CI: 7.62–14.79, TT II (arm B) = 9.5/kPY; 95%CI: 6.64–13.59, TT IIIA = 5.35/kPY; 95%CI: 3.28–8.73, TT IIIB = 7.87/kPY; 95%CI: 4.47–13.87, <i>p</i> = .6). The event rate of secondary solid cancers in patients who received tandem autologous HSCT was similar the only one transplant (IRR = 1.1, <i>p</i> = .8). Similarly, there was no difference in secondary solid cancers event rates between tandem and non-tandem double transplant (IRR = 0.88, <i>p</i> = .75). Details of secondary solid cancers according to protocol are summarized in Table S7.</p><p>At the 15-year median follow-up point, it was observed that the majority of surviving patients did not develop solid malignancies. The proportion of patients with secondary solid cancers at 15 years was as follows: 8.5% in TT I (95% CI: 1.6–14.8%), 15.7% in TT II (arm A) (95% CI: 11.1–20%), 13.6% in TT II (arm B) (95% CI: 9.8–18%), 8.2% in TT IIIA (95% CI: 3.7–12.5%), and 10.9% in TT IIIB (95% CI: 3.4–16%). Figure S7.</p><p>To our knowledge, this is the largest and most comprehensive analysis with the longest follow-up duration to report on risk of SPM in MM patients who underwent tandem autologous HSCT. The incidence of SHM and secondary solid malignancies in patients undergoing tandem autologous HSCT on earlier TT protocols, with a median follow-up exceeding 15 years, was relatively low at 6.8% and 8.6%, respectively. Our extended follow-up revealed a relatively low risk of developing MDS and/or AML and/or MDS/MPN of 4.4%.</p><p>The International Myeloma Working Group (IMWG) suggests an intensified monitoring approach and precise quantification of second cancers in the context of clinical trials, proposing the inclusion of SPM as a defined endpoint. With the improvement of OS, patients need to undergo age-appropriate cancer screening. Our study revealed that the most common secondary solid malignancies were prostate cancer, breast cancer, and colon cancer. Such cancers are common and there are various guidelines that support screening of the general population for early detection and/or intervention.</p><p>The emergence of SHM or secondary solid malignancy was correlated with worse OS. This underscores the importance of vigilance in monitoring and managing these complications. Our findings emphasize that autologous transplantation in MM, particularly tandem autologous transplant in our trials, led to a significant improvement in OS even before the era of anti-CD38 monoclonal antibodies, bispecific antibodies, and chimeric antigen T-cell receptor therapy. This implies that early consideration of autotransplant, especially in eligible patients, can positively influence long-term outcomes. Our analysis revealed no difference in the risk of SHM between patients undergoing single versus tandem autologous HSCT. The risk is relatively low for both types (5.6%) even with long follow-up duration (16.6 years). While tandem autologous HSCT is used less frequently nowadays, it is still considered as standard of care in high-risk MM per the European Hematology Association (EHA)-European Society for Medical Oncology (ESMO) Clinical Practice Guidelines. The National Comprehensive Cancer Network (NCCN) guidelines suggest that tandem autologous HSCT can be considered for all patients who are candidates for transplant and is an option for patients who done not achieve at least a very good partial response after first autologous HSCT and in high-risk MM. It is our practice to offer tandem autologous HSCT in young patients and patients with high-risk disease.<span><sup>6</sup></span></p><p>Clonal hematopoiesis of indeterminate potential (CHIP) is associated with a small risk of progression to MDS and/or AML. Its prevalence is higher in older populations and in patients who received chemotherapy.<span><sup>7</sup></span> Unfortunately, CHIP data are not available for our patients, so we cannot determine if the MDS and AML cases were a consequence of CHIP. In addition, CHIP was associated with poor OS and PFS in patients receiving HSCT for MM.<span><sup>8</sup></span></p><p>Tandem autologous HSCT was not associated with increased risk of SHM when compared with single autologous HSCT (6.8% vs. 4.3%) and no statistically significant difference in secondary solid malignancies (8.6% vs. 5.6%). Median OS was longer in patients who underwent tandem autologous HSCT: 10.88 years (95% CI: 9.85–11.74 years) compared with 6.08 years (95% CI: 4.58–7.74 years), <i>p</i>-value <.001. Although the tandem approach did not increase the rate of malignancies, we emphasize the need for rigorous screening in older MM patients, with specific recommendations for monitoring hematologic abnormalities and common solid tumors like breast, prostate, colorectal cancer, and melanoma according to established guidelines. Patients included were not treated with upfront novel agents such as anti-CD38 monoclonal antibodies, bispecific antibodies, or Chimeric Antigen Receptor T-cell (CAR T) cells, which have significantly changed the treatment landscape. Future trials will report on the risk of secondary malignancies associated with these new approaches.</p><p>In conclusion, our study comprehensively examines SPM in MM patients treated with autologous HSCT under various earlier TT protocols. The occurrence of SHM and secondary solid malignancies in patients treated with tandem autologous HSCT on earlier TT protocols and followed for a median of over 15 years was relatively low. Autologous HSCT in MM, particularly tandem autologous HSCT in our trials, significantly improved OS and should be offered early to eligible patients.</p><p><b>Conceived and designed the analysis:</b> SAH, CS, GT, ERS, BB, FVR. <b>Performed and assisted analysis:</b> SAH, OA, and E.RS. <b>Wrote the original draft of the paper:</b> SAH. <b>Reviewed and edited the paper:</b> All authors.</p><p>SAH reports receiving consulting fees from Jansen, Pfizer, and Sanofi.</p>\",\"PeriodicalId\":7724,\"journal\":{\"name\":\"American Journal of Hematology\",\"volume\":\"99 11\",\"pages\":\"2222-2224\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2024-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27452\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27452\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27452","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
74岁),P值为0.001。虽然串联方法没有增加恶性肿瘤的发生率,但我们强调需要对老年 MM 患者进行严格筛查,并根据既定指南提出监测血液学异常和常见实体瘤(如乳腺癌、前列腺癌、结直肠癌和黑色素瘤)的具体建议。纳入的患者未接受抗CD38单克隆抗体、双特异性抗体或嵌合抗原受体T细胞(CAR T)等新型药物的前期治疗,而这些药物已显著改变了治疗格局。总之,我们的研究全面考察了在各种早期 TT 方案下接受自体造血干细胞移植治疗的 MM 患者的 SPM。在早期TT方案下接受串联自体造血干细胞移植治疗并随访中位数超过15年的患者中,SHM和继发性实体恶性肿瘤的发生率相对较低。自体造血干细胞移植治疗MM,尤其是我们试验中的串联自体造血干细胞移植,可显著改善OS,应尽早向符合条件的患者提供:SAH、CS、GT、IERS、BB、FVR。执行并协助分析:SAH、OA和E.RS。撰写论文原稿:SAH:SAH。审阅并编辑论文:所有作者。SAH 报告称从 Jansen、辉瑞和赛诺菲获得咨询费。
Second primary malignancies after tandem autologous hematopoietic stem cell transplantation for multiple myeloma
Autologous hematopoietic stem cell transplantation (HSCT) is a standard treatment for eligible multiple myeloma (MM) patients.1 Before high-dose chemotherapy and autologous HSCT, patients typically receive induction therapy with a proteasome inhibitor and an immunomodulatory (IMiD) agent. This approach, along with posttransplant maintenance therapies, has improved survival, with some patients achieving a median overall survival (OS) of over 10 years.1
While late mortality rates have decreased over the past three decades, the incidence of second primary malignancies (SPM) has not.2 Given improved survival rates, understanding long-term complications like SPM is crucial, particularly as most phase III MM trials lack extended follow-up.3
Autologous HSCT enhances long-term disease control and survival in newly diagnosed MM patients but increases the risk of SPM, including second hematologic malignancies (SHM). A Swedish study found that higher cumulative doses of melphalan were linked to a 2.8-fold increased risk of therapy-related myeloid neoplasms.4 In a study of 3948 MM patients, 4% developed SPM, with 64% being solid tumors, 20% myeloid, 14% SHM, and 2% lymphoid malignancies. This study included only single autologous HSCT patients and had a median follow-up of 37 months, limiting the assessment of late SPM development.5
The principal objective of this study was to examine the occurrence and attributes of SPM and their subsequent effects on OS. Additionally, we sought to investigate whether the utilization of tandem autologous HSCT was associated with an elevated risk of SPM in comparison with single autologous HSCT. Secondary aims included the classification of various SPM types that emerged following autologous HSCT. Methods are detailed in supplementary.
A total of 1379 patients with newly diagnosed MM enrolled on four TT trials. An overview of the patients' characteristics can be found in [Table S1]. The median follow-up durations varied across different treatment groups: 25.3 years for TT I, 20.4 years for TT II (Arm A), 19.8 years for TT II (Arm B), 17.1 years for TT IIIA, and 15.4 years for TT IIIB. When considering the entire cohort of 1379 patients in the study, the median follow-up period was 16.6 years, with an interquartile range (IQR) spanning from 13.5 to 20 years. A total of 2640 transplants were performed on patients in our study cohort, with most of the transplants as first autologous HSCT (n = 1267) and second autologous HSCT (n = 1034) [Table S2]. Patients' baseline characteristics according to the type of transplant are summarized in [Table S3]. Overall, among the total of 1379 enrolled patients in the study, 974 patients (71%) underwent tandem autologous HSCT, with an average time interval of approximately 3.2 months between the first and second autologous HSCT [Table S4]. Event rates of SPM, characteristics of patients with more than one SPM, and survival analysis based on SPM are summarized in Supplementary (Figure S1–S6 and Table S5).
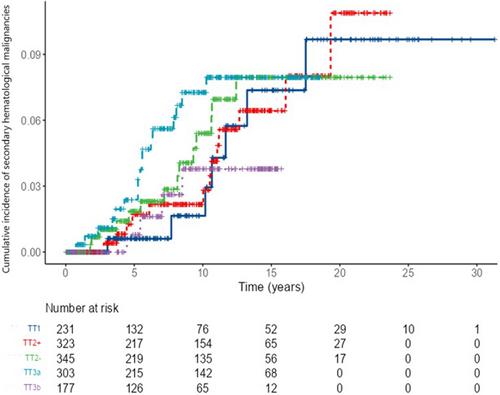
A total of 78 (5.6%) patients were diagnosed with any SHM. Myelodysplastic syndrome (MDS) alone, MDS with myeloproliferative neoplasms (MDS/MPN) and acute myelogenous leukemia (AML) occurred in 61 (4.4%) of patients. Acute lymphoblastic leukemia (ALL) occurred only in four (0.3%) of patients. A fitted Poisson regression was used to determine the event rate of SHM and the statistical differences between trials. There was a significant difference of SHM event rates between trials (TT I = 3.9/kPY; 95%CI: 2–7.8, TT II (Arm A) = 5.3/kPY; 95%CI: 3.3–8.6, TT II (Arm B) = 6.9/kPY; 95%CI: 4.5–10.6, TT IIIA = 9.3/kPY; 95%CI: 6.4–13.6, TT IIIB = 3.3/kPY; 95%CI: 1.4–7.9, p < .001). Based on pairwise comparisons, SHM event rates in TT I were similar compared with TT II (Arm A) (IRR = 0.44, p = .044), TT II (Arm B) (IRR = 0.61, p = .28), TT IIIA (IRR = 0.38, p = .017), and TT IIIB (IRR = 1.15, p = .77). TT IIIA SHM rate was similar to TT IIIB (IRR = 1.51, p = .29). Other event rates did not differ between trials (p > .01 for pairwise comparisons). The percentage of tandem autologous HSCT was higher in TT IIIA (85%) and TT IIIB (84%) when compared with TT I (59%), TT II (arm A) (65%) and TT II (Arm B) (65%) (chi-square p < .001). In addition, the event rate of SHM in patients who received tandem autologous HSCT was similar the only one transplant (IRR = 1.02, p = .99). It was also similar when comparing tandem with non-tandem double transplant (IRR = 0.47, p = .06). Based on a specific SHM type, no statistical difference was found between protocols. Details of SHM according to protocol are summarized in Table.S6.
At a median follow-up period of 15 years, the majority of surviving patients did not exhibit SHM. The proportion of patients with SHM at 15 years was as follows: 7.4% in the TT I group (95% CI: 1.3–13.1%), 6.4% in the TT II (arm A) group (95% CI: 2.5–10.1%), 8% in the TT II (arm B) group (95% CI: 3.6–12.1%), 8% in the TT IIIA group (95% CI: 4.2–11.6%), and 3.8% in the TT IIIB group (95% CI: 0–3.4%). Figure 1. RMTL analysis did not find a statistical difference between TT IIIA versus TT IIIB (p = .246) and tandem versus single transplant (p = .767).
Secondary solid cancers were observed in 7.6% of the study cohort, encompassing 105 cases out of a total of 1379 patients. Eight patients had more than one solid malignancy. The most prevalent secondary solid cancers were prostate cancer (22 tumors), breast cancer (15 tumors), and colorectal cancer (15 tumors). There was no significant difference of secondary solid cancers event rates between trials (TT I = 5.72/kPY; 95%CI: 3.25–10.08, TT II (arm A) = 10.62/kPY; 95%CI: 7.62–14.79, TT II (arm B) = 9.5/kPY; 95%CI: 6.64–13.59, TT IIIA = 5.35/kPY; 95%CI: 3.28–8.73, TT IIIB = 7.87/kPY; 95%CI: 4.47–13.87, p = .6). The event rate of secondary solid cancers in patients who received tandem autologous HSCT was similar the only one transplant (IRR = 1.1, p = .8). Similarly, there was no difference in secondary solid cancers event rates between tandem and non-tandem double transplant (IRR = 0.88, p = .75). Details of secondary solid cancers according to protocol are summarized in Table S7.
At the 15-year median follow-up point, it was observed that the majority of surviving patients did not develop solid malignancies. The proportion of patients with secondary solid cancers at 15 years was as follows: 8.5% in TT I (95% CI: 1.6–14.8%), 15.7% in TT II (arm A) (95% CI: 11.1–20%), 13.6% in TT II (arm B) (95% CI: 9.8–18%), 8.2% in TT IIIA (95% CI: 3.7–12.5%), and 10.9% in TT IIIB (95% CI: 3.4–16%). Figure S7.
To our knowledge, this is the largest and most comprehensive analysis with the longest follow-up duration to report on risk of SPM in MM patients who underwent tandem autologous HSCT. The incidence of SHM and secondary solid malignancies in patients undergoing tandem autologous HSCT on earlier TT protocols, with a median follow-up exceeding 15 years, was relatively low at 6.8% and 8.6%, respectively. Our extended follow-up revealed a relatively low risk of developing MDS and/or AML and/or MDS/MPN of 4.4%.
The International Myeloma Working Group (IMWG) suggests an intensified monitoring approach and precise quantification of second cancers in the context of clinical trials, proposing the inclusion of SPM as a defined endpoint. With the improvement of OS, patients need to undergo age-appropriate cancer screening. Our study revealed that the most common secondary solid malignancies were prostate cancer, breast cancer, and colon cancer. Such cancers are common and there are various guidelines that support screening of the general population for early detection and/or intervention.
The emergence of SHM or secondary solid malignancy was correlated with worse OS. This underscores the importance of vigilance in monitoring and managing these complications. Our findings emphasize that autologous transplantation in MM, particularly tandem autologous transplant in our trials, led to a significant improvement in OS even before the era of anti-CD38 monoclonal antibodies, bispecific antibodies, and chimeric antigen T-cell receptor therapy. This implies that early consideration of autotransplant, especially in eligible patients, can positively influence long-term outcomes. Our analysis revealed no difference in the risk of SHM between patients undergoing single versus tandem autologous HSCT. The risk is relatively low for both types (5.6%) even with long follow-up duration (16.6 years). While tandem autologous HSCT is used less frequently nowadays, it is still considered as standard of care in high-risk MM per the European Hematology Association (EHA)-European Society for Medical Oncology (ESMO) Clinical Practice Guidelines. The National Comprehensive Cancer Network (NCCN) guidelines suggest that tandem autologous HSCT can be considered for all patients who are candidates for transplant and is an option for patients who done not achieve at least a very good partial response after first autologous HSCT and in high-risk MM. It is our practice to offer tandem autologous HSCT in young patients and patients with high-risk disease.6
Clonal hematopoiesis of indeterminate potential (CHIP) is associated with a small risk of progression to MDS and/or AML. Its prevalence is higher in older populations and in patients who received chemotherapy.7 Unfortunately, CHIP data are not available for our patients, so we cannot determine if the MDS and AML cases were a consequence of CHIP. In addition, CHIP was associated with poor OS and PFS in patients receiving HSCT for MM.8
Tandem autologous HSCT was not associated with increased risk of SHM when compared with single autologous HSCT (6.8% vs. 4.3%) and no statistically significant difference in secondary solid malignancies (8.6% vs. 5.6%). Median OS was longer in patients who underwent tandem autologous HSCT: 10.88 years (95% CI: 9.85–11.74 years) compared with 6.08 years (95% CI: 4.58–7.74 years), p-value <.001. Although the tandem approach did not increase the rate of malignancies, we emphasize the need for rigorous screening in older MM patients, with specific recommendations for monitoring hematologic abnormalities and common solid tumors like breast, prostate, colorectal cancer, and melanoma according to established guidelines. Patients included were not treated with upfront novel agents such as anti-CD38 monoclonal antibodies, bispecific antibodies, or Chimeric Antigen Receptor T-cell (CAR T) cells, which have significantly changed the treatment landscape. Future trials will report on the risk of secondary malignancies associated with these new approaches.
In conclusion, our study comprehensively examines SPM in MM patients treated with autologous HSCT under various earlier TT protocols. The occurrence of SHM and secondary solid malignancies in patients treated with tandem autologous HSCT on earlier TT protocols and followed for a median of over 15 years was relatively low. Autologous HSCT in MM, particularly tandem autologous HSCT in our trials, significantly improved OS and should be offered early to eligible patients.
Conceived and designed the analysis: SAH, CS, GT, ERS, BB, FVR. Performed and assisted analysis: SAH, OA, and E.RS. Wrote the original draft of the paper: SAH. Reviewed and edited the paper: All authors.
SAH reports receiving consulting fees from Jansen, Pfizer, and Sanofi.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
