{"title":"西妥昔单抗每两周给药一次与标准每周给药一次在转移性结直肠癌中的临床非劣效性的模型信息证据","authors":"Ana-Marija Milenković-Grišić, Siobhán Hayes, Colm Farrell, Yoshihiro Kuroki, Mauro Bertolino, Karthik Venkatakrishnan, Pascal Girard","doi":"10.1002/cpt.3345","DOIUrl":null,"url":null,"abstract":"<p>Cetuximab was initially developed and approved as a first-line treatment in patients with unresectable metastatic colorectal cancer (mCRC) for weekly administration (250 mg/m<sup>2</sup> Q1W with 400 mg/m<sup>2</sup> loading dose). An every-2-weeks schedule (500 mg/m<sup>2</sup> Q2W) was approved recently by several health authorities. Being synchronized with chemotherapy, Q2W administration should improve patients' convenience and healthcare resource utilization. Herein, we present evidence of non-inferiority of Q2W cetuximab, compared with Q1W dosing using pharmacometrics modeling and clinical trial simulation (CTS). Pooled data from five phase I–III clinical trials in 852 patients with <i>KRAS</i> wild-type mCRC treated with Q1W or Q2W cetuximab were modeled using a population exposure–tumor size (TS) model linked to overall survival (OS); exposure was derived from a previously established population pharmacokinetic model. A semi-mechanistic TS model adapted from the Claret model incorporated killing rate proportional to cetuximab area under the concentration-time curve over 2 weeks (AUC) with Eastern Cooperative Oncology Group (ECOG) status as covariate on baseline TS. The OS was modeled with Weibull hazard using ECOG, baseline TS, primary tumor location, and predicted percent change in TS at 8 weeks as covariates. Model-based simulations revealed indistinguishable early tumor shrinkage and survival between Q2W vs. Q1W cetuximab. CTS evaluated OS non-inferiority (predefined margin of 1.25) in 1,000 trials, each with 2,000 virtual patients receiving Q2W or Q1W cetuximab (1:1), and demonstrated non-inferiority in 94% of cases. Taken together, these analyses provide model-based evidence for clinical non-inferiority of Q2W vs. Q1W cetuximab in mCRC with potential benefits to patients and healthcare providers.</p>","PeriodicalId":153,"journal":{"name":"Clinical Pharmacology & Therapeutics","volume":"116 4","pages":"1071-1081"},"PeriodicalIF":5.5000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cpt.3345","citationCount":"0","resultStr":"{\"title\":\"Model-informed Evidence for Clinical Non-inferiority of Every-2-Weeks Versus Standard Weekly Dosing Schedule of Cetuximab in Metastatic Colorectal Cancer\",\"authors\":\"Ana-Marija Milenković-Grišić, Siobhán Hayes, Colm Farrell, Yoshihiro Kuroki, Mauro Bertolino, Karthik Venkatakrishnan, Pascal Girard\",\"doi\":\"10.1002/cpt.3345\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Cetuximab was initially developed and approved as a first-line treatment in patients with unresectable metastatic colorectal cancer (mCRC) for weekly administration (250 mg/m<sup>2</sup> Q1W with 400 mg/m<sup>2</sup> loading dose). An every-2-weeks schedule (500 mg/m<sup>2</sup> Q2W) was approved recently by several health authorities. Being synchronized with chemotherapy, Q2W administration should improve patients' convenience and healthcare resource utilization. Herein, we present evidence of non-inferiority of Q2W cetuximab, compared with Q1W dosing using pharmacometrics modeling and clinical trial simulation (CTS). Pooled data from five phase I–III clinical trials in 852 patients with <i>KRAS</i> wild-type mCRC treated with Q1W or Q2W cetuximab were modeled using a population exposure–tumor size (TS) model linked to overall survival (OS); exposure was derived from a previously established population pharmacokinetic model. A semi-mechanistic TS model adapted from the Claret model incorporated killing rate proportional to cetuximab area under the concentration-time curve over 2 weeks (AUC) with Eastern Cooperative Oncology Group (ECOG) status as covariate on baseline TS. The OS was modeled with Weibull hazard using ECOG, baseline TS, primary tumor location, and predicted percent change in TS at 8 weeks as covariates. Model-based simulations revealed indistinguishable early tumor shrinkage and survival between Q2W vs. Q1W cetuximab. CTS evaluated OS non-inferiority (predefined margin of 1.25) in 1,000 trials, each with 2,000 virtual patients receiving Q2W or Q1W cetuximab (1:1), and demonstrated non-inferiority in 94% of cases. Taken together, these analyses provide model-based evidence for clinical non-inferiority of Q2W vs. Q1W cetuximab in mCRC with potential benefits to patients and healthcare providers.</p>\",\"PeriodicalId\":153,\"journal\":{\"name\":\"Clinical Pharmacology & Therapeutics\",\"volume\":\"116 4\",\"pages\":\"1071-1081\"},\"PeriodicalIF\":5.5000,\"publicationDate\":\"2024-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cpt.3345\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pharmacology & Therapeutics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://ascpt.onlinelibrary.wiley.com/doi/10.1002/cpt.3345\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacology & Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://ascpt.onlinelibrary.wiley.com/doi/10.1002/cpt.3345","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Model-informed Evidence for Clinical Non-inferiority of Every-2-Weeks Versus Standard Weekly Dosing Schedule of Cetuximab in Metastatic Colorectal Cancer
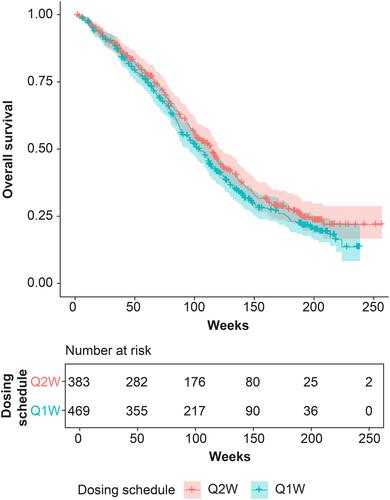
Cetuximab was initially developed and approved as a first-line treatment in patients with unresectable metastatic colorectal cancer (mCRC) for weekly administration (250 mg/m2 Q1W with 400 mg/m2 loading dose). An every-2-weeks schedule (500 mg/m2 Q2W) was approved recently by several health authorities. Being synchronized with chemotherapy, Q2W administration should improve patients' convenience and healthcare resource utilization. Herein, we present evidence of non-inferiority of Q2W cetuximab, compared with Q1W dosing using pharmacometrics modeling and clinical trial simulation (CTS). Pooled data from five phase I–III clinical trials in 852 patients with KRAS wild-type mCRC treated with Q1W or Q2W cetuximab were modeled using a population exposure–tumor size (TS) model linked to overall survival (OS); exposure was derived from a previously established population pharmacokinetic model. A semi-mechanistic TS model adapted from the Claret model incorporated killing rate proportional to cetuximab area under the concentration-time curve over 2 weeks (AUC) with Eastern Cooperative Oncology Group (ECOG) status as covariate on baseline TS. The OS was modeled with Weibull hazard using ECOG, baseline TS, primary tumor location, and predicted percent change in TS at 8 weeks as covariates. Model-based simulations revealed indistinguishable early tumor shrinkage and survival between Q2W vs. Q1W cetuximab. CTS evaluated OS non-inferiority (predefined margin of 1.25) in 1,000 trials, each with 2,000 virtual patients receiving Q2W or Q1W cetuximab (1:1), and demonstrated non-inferiority in 94% of cases. Taken together, these analyses provide model-based evidence for clinical non-inferiority of Q2W vs. Q1W cetuximab in mCRC with potential benefits to patients and healthcare providers.
期刊介绍:
Clinical Pharmacology & Therapeutics (CPT) is the authoritative cross-disciplinary journal in experimental and clinical medicine devoted to publishing advances in the nature, action, efficacy, and evaluation of therapeutics. CPT welcomes original Articles in the emerging areas of translational, predictive and personalized medicine; new therapeutic modalities including gene and cell therapies; pharmacogenomics, proteomics and metabolomics; bioinformation and applied systems biology complementing areas of pharmacokinetics and pharmacodynamics, human investigation and clinical trials, pharmacovigilence, pharmacoepidemiology, pharmacometrics, and population pharmacology.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
