Hartmut Döhner, Keith W Pratz, Courtney D DiNardo, Andrew H Wei, Brian A Jonas, Vinod A Pullarkat, Michael J Thirman, Christian Récher, Andre C Schuh, Sunil Babu, Xiaotong Li, Grace Ku, Zihuan Liu, Yan Sun, Jalaja Potluri, Monique Dail, Brenda Chyla, Daniel A Pollyea
{"title":"基因风险分层与接受 Venetoclax 和阿扎胞苷治疗的急性髓细胞性白血病无效患者的预后","authors":"Hartmut Döhner, Keith W Pratz, Courtney D DiNardo, Andrew H Wei, Brian A Jonas, Vinod A Pullarkat, Michael J Thirman, Christian Récher, Andre C Schuh, Sunil Babu, Xiaotong Li, Grace Ku, Zihuan Liu, Yan Sun, Jalaja Potluri, Monique Dail, Brenda Chyla, Daniel A Pollyea","doi":"10.1182/blood.2024024944","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong>The European LeukemiaNet (ELN) acute myeloid leukemia (AML) genetic risk classification systems are based on response to intensive chemotherapy; their ability to discriminate outcomes in older patients treated with venetoclax-azacitidine may be suboptimal. This pooled analysis of the phase 3 VIALE-A trial (NCT02993523) and phase 1b study (NCT02203773) examined prognostic stratification according to the 2017 and 2022 ELN risk classifications and derived new molecular signatures differentiating venetoclax-azacitidine-treated patients based on overall survival (OS). Overall, 279 patients treated with venetoclax-azacitidine and 113 patients treated with placebo-azacitidine were analyzed. The ELN 2017 or 2022 prognostic criteria classified most patients as adverse-risk AML (60.2% and 72.8% for venetoclax-azacitidine and 65.5% and 75.2% for placebo-azacitidine, respectively). Although outcomes with venetoclax-azacitidine improved across all ELN risk groups compared with placebo-azacitidine, ELN classification systems poorly discriminated venetoclax-azacitidine outcomes. By applying a bioinformatic algorithm, new molecular signatures were derived differentiating OS outcomes with venetoclax-azacitidine. The mutational status of TP53, FLT3 internal tandem duplication (FLT3-ITD), NRAS, and KRAS categorized patients into higher-, intermediate-, and lower-benefit groups (52%, 25%, and 23% of patients, respectively), each associated with a distinct median OS (26.5 months [95% confidence interval (CI), 20.2-32.7]; 12.1 months [95% CI, 7.3-15.2]; and 5.5 months [95% CI, 2.8-7.6], respectively). ELN prognostic classifiers did not provide clinically meaningful risk stratification of OS outcomes in patients treated with venetoclax-azacitidine. TP53, FLT3-ITD, NRAS, and KRAS mutation status allows the classification of these patients into 3 risk groups with distinct differences in median OS. These trials were registered at www.clinicaltrials.gov as #NCT02993523 and #NCT02203773.</p>","PeriodicalId":9102,"journal":{"name":"Blood","volume":" ","pages":"2211-2222"},"PeriodicalIF":23.9000,"publicationDate":"2024-11-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11600046/pdf/","citationCount":"0","resultStr":"{\"title\":\"Genetic risk stratification and outcomes among treatment-naive patients with AML treated with venetoclax and azacitidine.\",\"authors\":\"Hartmut Döhner, Keith W Pratz, Courtney D DiNardo, Andrew H Wei, Brian A Jonas, Vinod A Pullarkat, Michael J Thirman, Christian Récher, Andre C Schuh, Sunil Babu, Xiaotong Li, Grace Ku, Zihuan Liu, Yan Sun, Jalaja Potluri, Monique Dail, Brenda Chyla, Daniel A Pollyea\",\"doi\":\"10.1182/blood.2024024944\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Abstract: </strong>The European LeukemiaNet (ELN) acute myeloid leukemia (AML) genetic risk classification systems are based on response to intensive chemotherapy; their ability to discriminate outcomes in older patients treated with venetoclax-azacitidine may be suboptimal. This pooled analysis of the phase 3 VIALE-A trial (NCT02993523) and phase 1b study (NCT02203773) examined prognostic stratification according to the 2017 and 2022 ELN risk classifications and derived new molecular signatures differentiating venetoclax-azacitidine-treated patients based on overall survival (OS). Overall, 279 patients treated with venetoclax-azacitidine and 113 patients treated with placebo-azacitidine were analyzed. The ELN 2017 or 2022 prognostic criteria classified most patients as adverse-risk AML (60.2% and 72.8% for venetoclax-azacitidine and 65.5% and 75.2% for placebo-azacitidine, respectively). Although outcomes with venetoclax-azacitidine improved across all ELN risk groups compared with placebo-azacitidine, ELN classification systems poorly discriminated venetoclax-azacitidine outcomes. By applying a bioinformatic algorithm, new molecular signatures were derived differentiating OS outcomes with venetoclax-azacitidine. The mutational status of TP53, FLT3 internal tandem duplication (FLT3-ITD), NRAS, and KRAS categorized patients into higher-, intermediate-, and lower-benefit groups (52%, 25%, and 23% of patients, respectively), each associated with a distinct median OS (26.5 months [95% confidence interval (CI), 20.2-32.7]; 12.1 months [95% CI, 7.3-15.2]; and 5.5 months [95% CI, 2.8-7.6], respectively). ELN prognostic classifiers did not provide clinically meaningful risk stratification of OS outcomes in patients treated with venetoclax-azacitidine. TP53, FLT3-ITD, NRAS, and KRAS mutation status allows the classification of these patients into 3 risk groups with distinct differences in median OS. These trials were registered at www.clinicaltrials.gov as #NCT02993523 and #NCT02203773.</p>\",\"PeriodicalId\":9102,\"journal\":{\"name\":\"Blood\",\"volume\":\" \",\"pages\":\"2211-2222\"},\"PeriodicalIF\":23.9000,\"publicationDate\":\"2024-11-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11600046/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1182/blood.2024024944\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1182/blood.2024024944","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
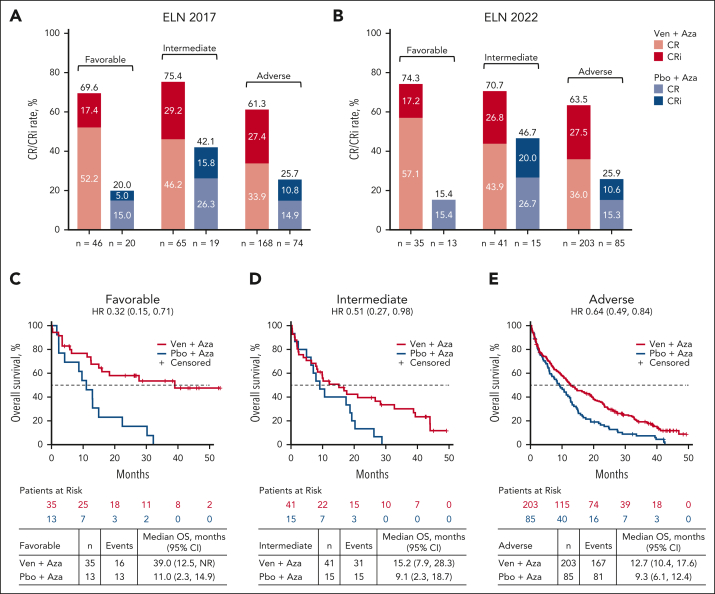
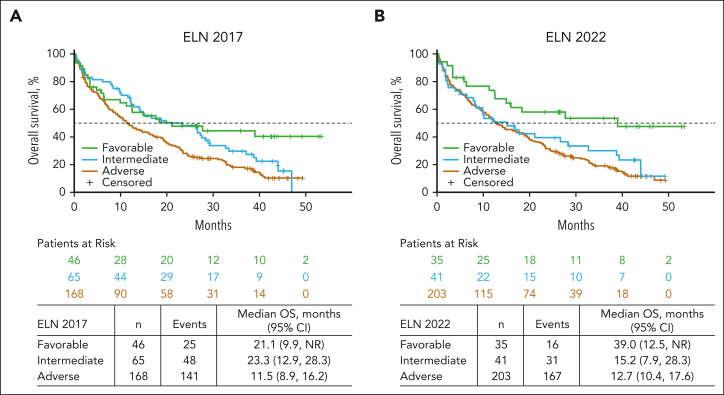
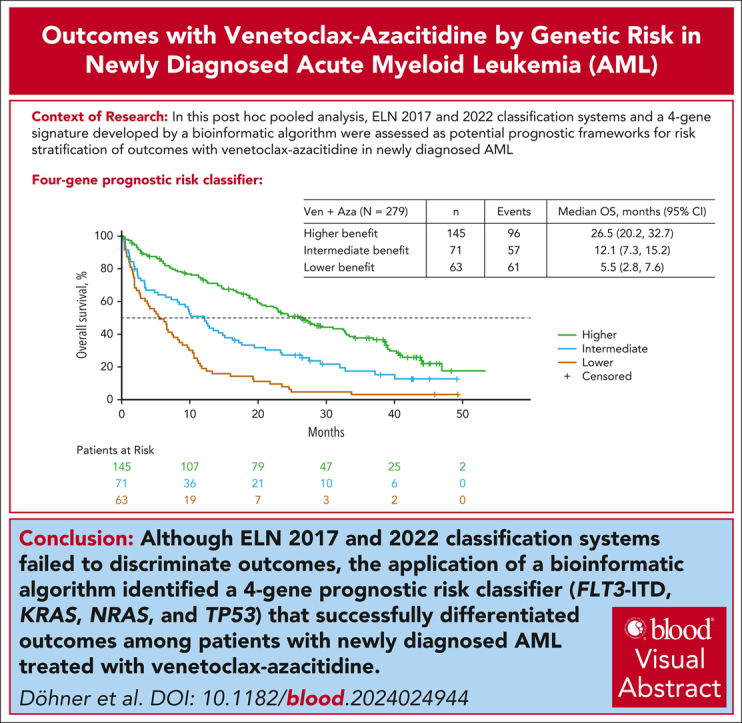
欧洲白血病网(ELN)急性髓性白血病(AML)遗传风险分级系统是基于对强化化疗的反应而建立的;它们对接受venetoclax-azacitidine治疗的老年患者的预后判别能力可能不够理想。在此,对3期VIALE-A试验(NCT02993523)和1b期研究(NCT02203773)中的患者进行了汇总分析,根据2017年和2022年ELN风险分类对预后分层进行了研究。一种生物信息学算法根据中位总生存期(OS)得出了新的分子特征,以区分接受venetoclax-阿扎胞苷治疗的患者。对279例接受venetoclax-阿扎胞苷治疗的患者和113例接受安慰剂-阿扎胞苷治疗的患者进行了分析。如果按照ELN 2017或2022预后标准进行分类,大多数患者属于不良风险急性髓细胞性白血病(venetoclax-azacitidine分别为60.2%和72.8%,placebo-azacitidine分别为65.5%和75.2%)。与安慰剂-阿扎胞苷相比,文尼氯雷-阿扎胞苷在所有ELN风险组中的疗效均有所改善,但ELN分类系统对文尼氯雷-阿扎胞苷疗效的判别能力较差。通过应用生物信息学算法,得出了新的分子特征来区分 Venetoclax-azacitidine 的 OS 结果;TP53、FLT3-ITD、NRAS 和 KRAS 的突变状态将患者分为高、中、低受益组(分别占患者的 52%、25% 和 23%),每组都与不同的中位 OS 相关(26.5个月[95% CI,20.2至32.7]、12.1个月[95% CI,7.3至15.2]和5.5个月[95% CI,2.8至7.6])。ELN预后分类器不能为接受venetoclax-azacitidine治疗的急性髓细胞性白血病患者的OS结果提供有临床意义的风险分层。TP53、FLT3-ITD、NRAS和KRAS突变状态可将这些患者分为三个风险组,其中位OS存在明显差异。
Genetic risk stratification and outcomes among treatment-naive patients with AML treated with venetoclax and azacitidine.
Abstract: The European LeukemiaNet (ELN) acute myeloid leukemia (AML) genetic risk classification systems are based on response to intensive chemotherapy; their ability to discriminate outcomes in older patients treated with venetoclax-azacitidine may be suboptimal. This pooled analysis of the phase 3 VIALE-A trial (NCT02993523) and phase 1b study (NCT02203773) examined prognostic stratification according to the 2017 and 2022 ELN risk classifications and derived new molecular signatures differentiating venetoclax-azacitidine-treated patients based on overall survival (OS). Overall, 279 patients treated with venetoclax-azacitidine and 113 patients treated with placebo-azacitidine were analyzed. The ELN 2017 or 2022 prognostic criteria classified most patients as adverse-risk AML (60.2% and 72.8% for venetoclax-azacitidine and 65.5% and 75.2% for placebo-azacitidine, respectively). Although outcomes with venetoclax-azacitidine improved across all ELN risk groups compared with placebo-azacitidine, ELN classification systems poorly discriminated venetoclax-azacitidine outcomes. By applying a bioinformatic algorithm, new molecular signatures were derived differentiating OS outcomes with venetoclax-azacitidine. The mutational status of TP53, FLT3 internal tandem duplication (FLT3-ITD), NRAS, and KRAS categorized patients into higher-, intermediate-, and lower-benefit groups (52%, 25%, and 23% of patients, respectively), each associated with a distinct median OS (26.5 months [95% confidence interval (CI), 20.2-32.7]; 12.1 months [95% CI, 7.3-15.2]; and 5.5 months [95% CI, 2.8-7.6], respectively). ELN prognostic classifiers did not provide clinically meaningful risk stratification of OS outcomes in patients treated with venetoclax-azacitidine. TP53, FLT3-ITD, NRAS, and KRAS mutation status allows the classification of these patients into 3 risk groups with distinct differences in median OS. These trials were registered at www.clinicaltrials.gov as #NCT02993523 and #NCT02203773.
期刊介绍:
Blood, the official journal of the American Society of Hematology, published online and in print, provides an international forum for the publication of original articles describing basic laboratory, translational, and clinical investigations in hematology. Primary research articles will be published under the following scientific categories: Clinical Trials and Observations; Gene Therapy; Hematopoiesis and Stem Cells; Immunobiology and Immunotherapy scope; Myeloid Neoplasia; Lymphoid Neoplasia; Phagocytes, Granulocytes and Myelopoiesis; Platelets and Thrombopoiesis; Red Cells, Iron and Erythropoiesis; Thrombosis and Hemostasis; Transfusion Medicine; Transplantation; and Vascular Biology. Papers can be listed under more than one category as appropriate.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
