Casper van der Zee, Jennifer Chang-Wolf, Marc A Koopmanschap, Redmer van Leeuwen, Robert Pl Wisse
{"title":"评估远程医疗的碳足迹:系统回顾。","authors":"Casper van der Zee, Jennifer Chang-Wolf, Marc A Koopmanschap, Redmer van Leeuwen, Robert Pl Wisse","doi":"10.1177/11786329241271562","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Healthcare is responsible for 4% to 10% of carbon emissions worldwide, of which 22% is related to transport. Telemedicine emerged as a potential solution to reduce the footprint, for example, by reducing travel. However, a need to understand which variables to include in carbon footprint estimations in telemedicine limits our understanding of the beneficial impact telemedicine might have on our environment. This paper aims to systematically assess the reported carbon footprint and include variables assessed by the literature, comparing telemedicine with usual care.</p><p><strong>Methods: </strong>The systematic review followed the PRISMA guidelines in PubMed, Medline, Embase and Scopus. A quality assessment was performed using a transparency checklist for carbon footprint calculators. Carbon emissions were evaluated based on four categories, including patient travel, and streamlined life cycle assessment (LCA) for assessing included variables relevant to telemedicine.</p><p><strong>Results: </strong>We included 33 articles from 1117 records for analysis. The average transparency score was 38% (range 18%-68%). The median roundtrip travel distance for each patient was 131 km (interquartile range [IQR]: 60.8-351), or 25.6 kgCO<sub>2</sub> (IQR: 10.6-105.6) emissions. There is high variance among included variables. Saved emissions are structurally underestimated by not including external factors such as a streamlined LCA.</p><p><strong>Conclusions: </strong>Telemedicine aids in reducing emissions, with travel distance being the most significant contributor. Additionally, we recommend accounting for the LCA since it highlights important nuances. This review furthers the debate on assessing carbon footprint savings due to telemedicine.</p>","PeriodicalId":12876,"journal":{"name":"Health Services Insights","volume":"17 ","pages":"11786329241271562"},"PeriodicalIF":2.1000,"publicationDate":"2024-08-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11320403/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessing the Carbon Footprint of Telemedicine: A Systematic Review.\",\"authors\":\"Casper van der Zee, Jennifer Chang-Wolf, Marc A Koopmanschap, Redmer van Leeuwen, Robert Pl Wisse\",\"doi\":\"10.1177/11786329241271562\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Healthcare is responsible for 4% to 10% of carbon emissions worldwide, of which 22% is related to transport. Telemedicine emerged as a potential solution to reduce the footprint, for example, by reducing travel. However, a need to understand which variables to include in carbon footprint estimations in telemedicine limits our understanding of the beneficial impact telemedicine might have on our environment. This paper aims to systematically assess the reported carbon footprint and include variables assessed by the literature, comparing telemedicine with usual care.</p><p><strong>Methods: </strong>The systematic review followed the PRISMA guidelines in PubMed, Medline, Embase and Scopus. A quality assessment was performed using a transparency checklist for carbon footprint calculators. Carbon emissions were evaluated based on four categories, including patient travel, and streamlined life cycle assessment (LCA) for assessing included variables relevant to telemedicine.</p><p><strong>Results: </strong>We included 33 articles from 1117 records for analysis. The average transparency score was 38% (range 18%-68%). The median roundtrip travel distance for each patient was 131 km (interquartile range [IQR]: 60.8-351), or 25.6 kgCO<sub>2</sub> (IQR: 10.6-105.6) emissions. There is high variance among included variables. Saved emissions are structurally underestimated by not including external factors such as a streamlined LCA.</p><p><strong>Conclusions: </strong>Telemedicine aids in reducing emissions, with travel distance being the most significant contributor. Additionally, we recommend accounting for the LCA since it highlights important nuances. This review furthers the debate on assessing carbon footprint savings due to telemedicine.</p>\",\"PeriodicalId\":12876,\"journal\":{\"name\":\"Health Services Insights\",\"volume\":\"17 \",\"pages\":\"11786329241271562\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-08-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11320403/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health Services Insights\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11786329241271562\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11786329241271562","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Assessing the Carbon Footprint of Telemedicine: A Systematic Review.
Background: Healthcare is responsible for 4% to 10% of carbon emissions worldwide, of which 22% is related to transport. Telemedicine emerged as a potential solution to reduce the footprint, for example, by reducing travel. However, a need to understand which variables to include in carbon footprint estimations in telemedicine limits our understanding of the beneficial impact telemedicine might have on our environment. This paper aims to systematically assess the reported carbon footprint and include variables assessed by the literature, comparing telemedicine with usual care.
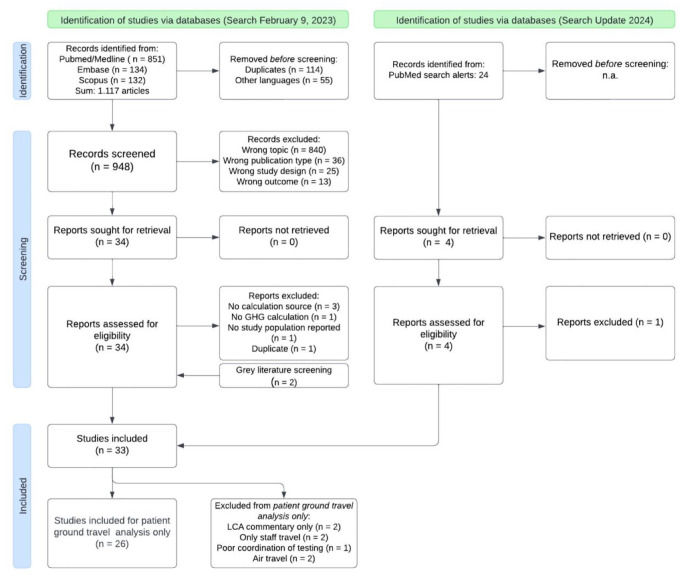
Methods: The systematic review followed the PRISMA guidelines in PubMed, Medline, Embase and Scopus. A quality assessment was performed using a transparency checklist for carbon footprint calculators. Carbon emissions were evaluated based on four categories, including patient travel, and streamlined life cycle assessment (LCA) for assessing included variables relevant to telemedicine.
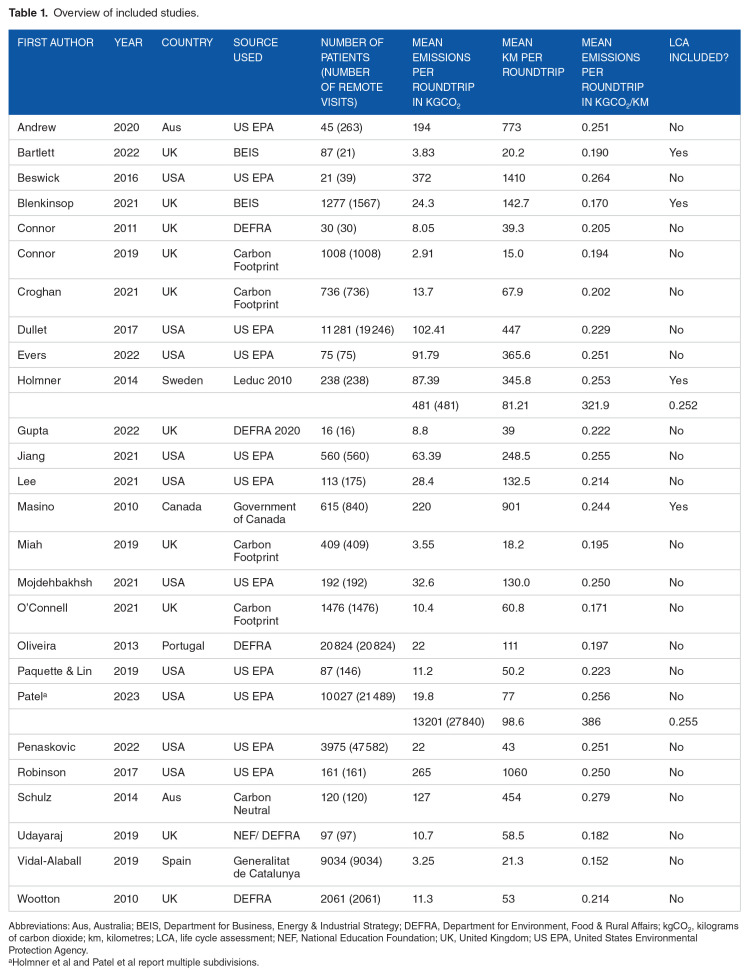
Results: We included 33 articles from 1117 records for analysis. The average transparency score was 38% (range 18%-68%). The median roundtrip travel distance for each patient was 131 km (interquartile range [IQR]: 60.8-351), or 25.6 kgCO2 (IQR: 10.6-105.6) emissions. There is high variance among included variables. Saved emissions are structurally underestimated by not including external factors such as a streamlined LCA.
Conclusions: Telemedicine aids in reducing emissions, with travel distance being the most significant contributor. Additionally, we recommend accounting for the LCA since it highlights important nuances. This review furthers the debate on assessing carbon footprint savings due to telemedicine.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
