Sungmin Zo, Ji-Yong Moon, Kyung Hoon Min, Hyun Lee
{"title":"继发性免疫缺陷和非囊性纤维化支气管扩张症。","authors":"Sungmin Zo, Ji-Yong Moon, Kyung Hoon Min, Hyun Lee","doi":"10.4046/trd.2024.0015","DOIUrl":null,"url":null,"abstract":"<p><p>Bronchiectasis is a chronic respiratory disease characterized by abnormal dilation of the bronchi that causes cough, sputum, and recurrent infections. As it may be associated with various respiratory or systemic diseases, a critical aspect of managing bronchiectasis is to identify the underlying cause. Immunodeficiency is a rare but important cause of bronchiectasis, and its treatability is a significant trait for bronchiectasis management. While primary immunodeficiencies in bronchiectasis are well recognized, secondary immunodeficiencies remain under-reported and under-researched. Secondary immunodeficiencies may result from various diseases and conditions, such as hematologic malignancies, human immunodeficiency virus infection, renal transplantation, or the use of immunosuppressive drugs, and may contribute to the occurrence of bronchiectasis. Recurrent pulmonary and/or extrapulmonary infections in bronchiectasis may indicate the presence of secondary immunodeficiency in patients with these underlying conditions. For treatment, examining the underlying condition, managing bronchiectasis adequately, and prophylactic antibiotics (e.g., macrolide) and/or supplementary immunoglobulin G therapy may provide potential benefits. Considering the projected increase in the prevalence of secondary immunodeficiencies and bronchiectasis, future guidelines and research on the diagnosis and optimized treatment are needed.</p>","PeriodicalId":23368,"journal":{"name":"Tuberculosis and Respiratory Diseases","volume":" ","pages":"440-450"},"PeriodicalIF":3.0000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11468440/pdf/","citationCount":"0","resultStr":"{\"title\":\"Secondary Immunodeficiency and Non-cystic Fibrosis Bronchiectasis.\",\"authors\":\"Sungmin Zo, Ji-Yong Moon, Kyung Hoon Min, Hyun Lee\",\"doi\":\"10.4046/trd.2024.0015\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Bronchiectasis is a chronic respiratory disease characterized by abnormal dilation of the bronchi that causes cough, sputum, and recurrent infections. As it may be associated with various respiratory or systemic diseases, a critical aspect of managing bronchiectasis is to identify the underlying cause. Immunodeficiency is a rare but important cause of bronchiectasis, and its treatability is a significant trait for bronchiectasis management. While primary immunodeficiencies in bronchiectasis are well recognized, secondary immunodeficiencies remain under-reported and under-researched. Secondary immunodeficiencies may result from various diseases and conditions, such as hematologic malignancies, human immunodeficiency virus infection, renal transplantation, or the use of immunosuppressive drugs, and may contribute to the occurrence of bronchiectasis. Recurrent pulmonary and/or extrapulmonary infections in bronchiectasis may indicate the presence of secondary immunodeficiency in patients with these underlying conditions. For treatment, examining the underlying condition, managing bronchiectasis adequately, and prophylactic antibiotics (e.g., macrolide) and/or supplementary immunoglobulin G therapy may provide potential benefits. Considering the projected increase in the prevalence of secondary immunodeficiencies and bronchiectasis, future guidelines and research on the diagnosis and optimized treatment are needed.</p>\",\"PeriodicalId\":23368,\"journal\":{\"name\":\"Tuberculosis and Respiratory Diseases\",\"volume\":\" \",\"pages\":\"440-450\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11468440/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tuberculosis and Respiratory Diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4046/trd.2024.0015\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tuberculosis and Respiratory Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4046/trd.2024.0015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
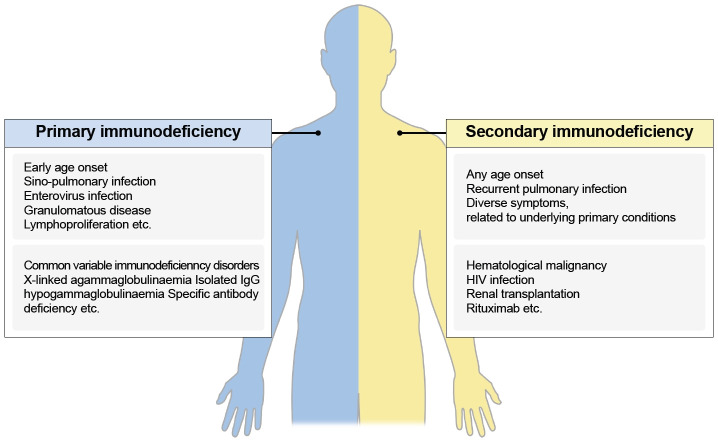
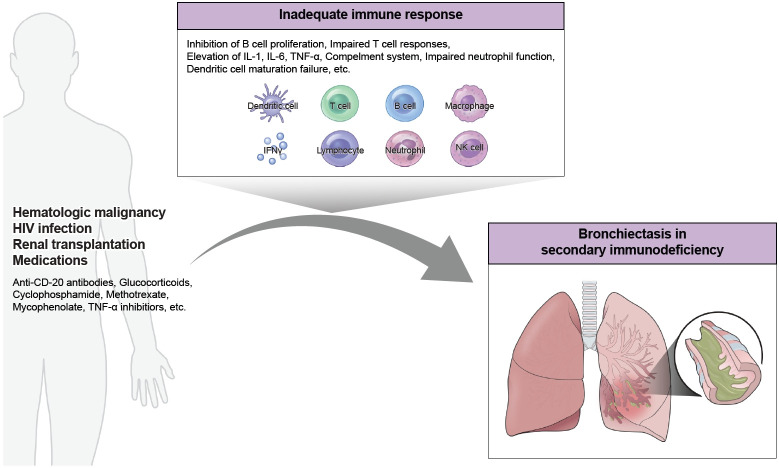
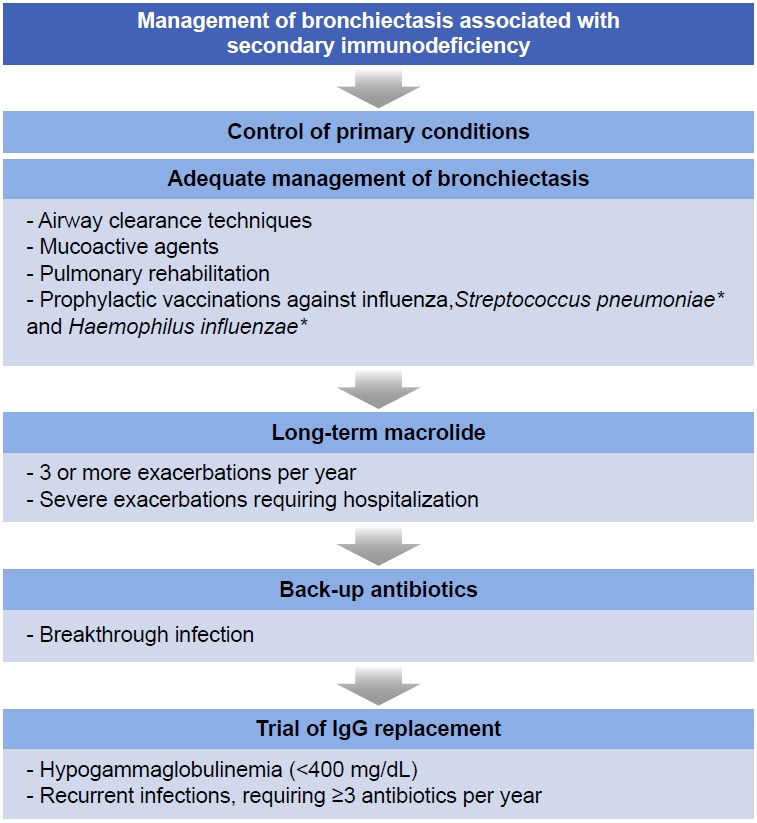
支气管扩张症是一种慢性呼吸道疾病,其特点是支气管异常扩张,导致咳嗽、咳痰和反复感染。由于支气管扩张症可能与各种呼吸系统或全身性疾病有关,因此查明病因是治疗支气管扩张症的关键。免疫缺陷是支气管扩张症的一个罕见但重要的病因,其可治疗性是支气管扩张症治疗的一个重要特征。支气管扩张症的原发性免疫缺陷已得到广泛认可,但继发性免疫缺陷的报道和研究仍然不足。继发性免疫缺陷可能由各种疾病和病症引起,如血液系统恶性肿瘤、人类免疫缺陷病毒感染、肾移植和使用免疫抑制剂,这些都可能导致支气管扩张的发生。支气管扩张症患者反复发生肺部和/或肺外感染,可能表明这些基础疾病患者存在继发性免疫缺陷。在治疗方面,检查基础疾病、充分控制支气管扩张、预防性使用抗生素(如大环内酯类)和/或补充免疫球蛋白 G 治疗可能会带来潜在的益处。考虑到继发性免疫缺陷和支气管扩张症的发病率预计会增加,未来需要制定有关诊断和优化治疗的指南并开展相关研究。
Secondary Immunodeficiency and Non-cystic Fibrosis Bronchiectasis.
Bronchiectasis is a chronic respiratory disease characterized by abnormal dilation of the bronchi that causes cough, sputum, and recurrent infections. As it may be associated with various respiratory or systemic diseases, a critical aspect of managing bronchiectasis is to identify the underlying cause. Immunodeficiency is a rare but important cause of bronchiectasis, and its treatability is a significant trait for bronchiectasis management. While primary immunodeficiencies in bronchiectasis are well recognized, secondary immunodeficiencies remain under-reported and under-researched. Secondary immunodeficiencies may result from various diseases and conditions, such as hematologic malignancies, human immunodeficiency virus infection, renal transplantation, or the use of immunosuppressive drugs, and may contribute to the occurrence of bronchiectasis. Recurrent pulmonary and/or extrapulmonary infections in bronchiectasis may indicate the presence of secondary immunodeficiency in patients with these underlying conditions. For treatment, examining the underlying condition, managing bronchiectasis adequately, and prophylactic antibiotics (e.g., macrolide) and/or supplementary immunoglobulin G therapy may provide potential benefits. Considering the projected increase in the prevalence of secondary immunodeficiencies and bronchiectasis, future guidelines and research on the diagnosis and optimized treatment are needed.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
