Reichling St Sauveur MD, Rodney Sufra MD, Marie Christine Jean Pierre MD, Vanessa Rouzier MD, Fabiola Preval RN, Serfine Exantus RN, Mirline Jean RN, Josette Jean PharmD, Guyrlaine Pierre-Louise Forestal PharmD, Obed Fleurijean BS, Nour Mourra BS, Anju Ogyu MPH, Rodolphe Malebranche MD, Jean Pierre Brisma MD, Marie M. Deschamps MD, Jean W. Pape MD, Radhika Sundararajan MD, PhD, Margaret L. McNairy MD, Msc, Lily D. Yan MD, Msc
{"title":"以社区为基础的高血压管理对海地城市贫民区高血压的影响:混合方法研究。","authors":"Reichling St Sauveur MD, Rodney Sufra MD, Marie Christine Jean Pierre MD, Vanessa Rouzier MD, Fabiola Preval RN, Serfine Exantus RN, Mirline Jean RN, Josette Jean PharmD, Guyrlaine Pierre-Louise Forestal PharmD, Obed Fleurijean BS, Nour Mourra BS, Anju Ogyu MPH, Rodolphe Malebranche MD, Jean Pierre Brisma MD, Marie M. Deschamps MD, Jean W. Pape MD, Radhika Sundararajan MD, PhD, Margaret L. McNairy MD, Msc, Lily D. Yan MD, Msc","doi":"10.1111/jch.14882","DOIUrl":null,"url":null,"abstract":"<p>Hypertension is a leading contributor to mortality in low-middle income countries including Haiti, yet only 13% achieve blood pressure (BP) control. We evaluated the effectiveness of a community-based hypertension management program delivered by community health workers (CHWs) and physicians among 100 adults with uncontrolled hypertension from the Haiti Cardiovascular Disease Cohort. The 12-month intervention included: community follow-up visits with CHWs (1 month if BP uncontrolled ≥140/90, 3 months otherwise) for BP measurement, lifestyle counseling, medication delivery, and dose adjustments. Primary outcome was mean change in systolic BP from enrollment to 12 months. Secondary outcomes were mean change in diastolic BP, BP control, acceptability, feasibility, and adverse events. We compared outcomes to 100 age, sex, and baseline BP matched controls with standard of care: clinic follow-up visits with physicians every 3 months. We also conducted qualitative interviews with participants and providers. Among 200 adults, median age was 59 years, 59% were female. Baseline mean BP was 154/89 mmHg intervention versus 153/88 mmHg control. At 12 months, the difference in SBP change between groups was −12.8 mmHg (95%CI −6.9, −18.7) and for DBP −7.1 mmHg (95%CI −3.3, −11.0). BP control increased from 0% to 58.1% in intervention, and 28.4% in control group. Four participants reported mild adverse events. In mixed methods analysis, we found community-based delivery addressed multiple participant barriers to care, and task-shifting with strong teamwork enhanced medication adherence. Community-based hypertension management using task-shifting with CHWs and community-based care was acceptable, and effective in reducing SBP, DBP, and increasing BP control.</p>","PeriodicalId":50237,"journal":{"name":"Journal of Clinical Hypertension","volume":"26 10","pages":"1133-1144"},"PeriodicalIF":2.5000,"publicationDate":"2024-08-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11466359/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effectiveness of community-based hypertension management on hypertension in the urban slums of Haiti: A mixed methods study\",\"authors\":\"Reichling St Sauveur MD, Rodney Sufra MD, Marie Christine Jean Pierre MD, Vanessa Rouzier MD, Fabiola Preval RN, Serfine Exantus RN, Mirline Jean RN, Josette Jean PharmD, Guyrlaine Pierre-Louise Forestal PharmD, Obed Fleurijean BS, Nour Mourra BS, Anju Ogyu MPH, Rodolphe Malebranche MD, Jean Pierre Brisma MD, Marie M. Deschamps MD, Jean W. Pape MD, Radhika Sundararajan MD, PhD, Margaret L. McNairy MD, Msc, Lily D. Yan MD, Msc\",\"doi\":\"10.1111/jch.14882\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Hypertension is a leading contributor to mortality in low-middle income countries including Haiti, yet only 13% achieve blood pressure (BP) control. We evaluated the effectiveness of a community-based hypertension management program delivered by community health workers (CHWs) and physicians among 100 adults with uncontrolled hypertension from the Haiti Cardiovascular Disease Cohort. The 12-month intervention included: community follow-up visits with CHWs (1 month if BP uncontrolled ≥140/90, 3 months otherwise) for BP measurement, lifestyle counseling, medication delivery, and dose adjustments. Primary outcome was mean change in systolic BP from enrollment to 12 months. Secondary outcomes were mean change in diastolic BP, BP control, acceptability, feasibility, and adverse events. We compared outcomes to 100 age, sex, and baseline BP matched controls with standard of care: clinic follow-up visits with physicians every 3 months. We also conducted qualitative interviews with participants and providers. Among 200 adults, median age was 59 years, 59% were female. Baseline mean BP was 154/89 mmHg intervention versus 153/88 mmHg control. At 12 months, the difference in SBP change between groups was −12.8 mmHg (95%CI −6.9, −18.7) and for DBP −7.1 mmHg (95%CI −3.3, −11.0). BP control increased from 0% to 58.1% in intervention, and 28.4% in control group. Four participants reported mild adverse events. In mixed methods analysis, we found community-based delivery addressed multiple participant barriers to care, and task-shifting with strong teamwork enhanced medication adherence. Community-based hypertension management using task-shifting with CHWs and community-based care was acceptable, and effective in reducing SBP, DBP, and increasing BP control.</p>\",\"PeriodicalId\":50237,\"journal\":{\"name\":\"Journal of Clinical Hypertension\",\"volume\":\"26 10\",\"pages\":\"1133-1144\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-08-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11466359/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Hypertension\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jch.14882\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Hypertension","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jch.14882","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Effectiveness of community-based hypertension management on hypertension in the urban slums of Haiti: A mixed methods study
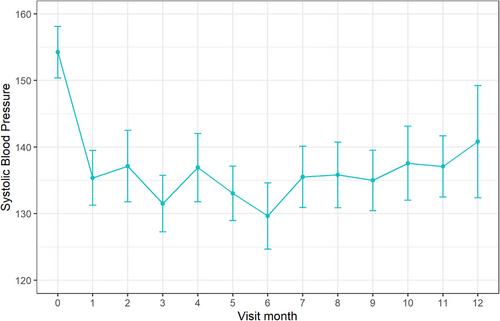
Hypertension is a leading contributor to mortality in low-middle income countries including Haiti, yet only 13% achieve blood pressure (BP) control. We evaluated the effectiveness of a community-based hypertension management program delivered by community health workers (CHWs) and physicians among 100 adults with uncontrolled hypertension from the Haiti Cardiovascular Disease Cohort. The 12-month intervention included: community follow-up visits with CHWs (1 month if BP uncontrolled ≥140/90, 3 months otherwise) for BP measurement, lifestyle counseling, medication delivery, and dose adjustments. Primary outcome was mean change in systolic BP from enrollment to 12 months. Secondary outcomes were mean change in diastolic BP, BP control, acceptability, feasibility, and adverse events. We compared outcomes to 100 age, sex, and baseline BP matched controls with standard of care: clinic follow-up visits with physicians every 3 months. We also conducted qualitative interviews with participants and providers. Among 200 adults, median age was 59 years, 59% were female. Baseline mean BP was 154/89 mmHg intervention versus 153/88 mmHg control. At 12 months, the difference in SBP change between groups was −12.8 mmHg (95%CI −6.9, −18.7) and for DBP −7.1 mmHg (95%CI −3.3, −11.0). BP control increased from 0% to 58.1% in intervention, and 28.4% in control group. Four participants reported mild adverse events. In mixed methods analysis, we found community-based delivery addressed multiple participant barriers to care, and task-shifting with strong teamwork enhanced medication adherence. Community-based hypertension management using task-shifting with CHWs and community-based care was acceptable, and effective in reducing SBP, DBP, and increasing BP control.
期刊介绍:
The Journal of Clinical Hypertension is a peer-reviewed, monthly publication that serves internists, cardiologists, nephrologists, endocrinologists, hypertension specialists, primary care practitioners, pharmacists and all professionals interested in hypertension by providing objective, up-to-date information and practical recommendations on the full range of clinical aspects of hypertension. Commentaries and columns by experts in the field provide further insights into our original research articles as well as on major articles published elsewhere. Major guidelines for the management of hypertension are also an important feature of the Journal. Through its partnership with the World Hypertension League, JCH will include a new focus on hypertension and public health, including major policy issues, that features research and reviews related to disease characteristics and management at the population level.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
