{"title":"对 LA-NSCLC 进行平行探索:化疗剂量-反应优化,同时考虑免疫疗法和减轻心脏毒性。","authors":"Huei-Tyng Huang","doi":"10.1016/j.radonc.2024.110477","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and purpose</h3><p>Chemoradiotherapy (CRT) for locally-advanced non-small cell lung cancer (LA-NSCLC) has undergone advances, including increased overall survival (OS) when combined with immune checkpoint blockade (ICB), and using cardiac-sparing techniques to reduce the radiotoxicity. This research investigated 1) how radiotherapy schedules can be optimised with CRT-ICB schemes, and 2) how cardiac-sparing might change the OS for concurrent CRT (cCRT).</p></div><div><h3>Methods and materials</h3><p>Survival data and dosimetric indices were sourced from published studies, with 2-year OS standardised and the hazard ratio of mean heart dose (MHD) against radiotoxicity tabulated in purpose. A published CRT dose–response model was selected, then modified with ICB and cardiac-sparing hypotheses. Models were maximum likelihood fitted, then visualised the prediction outcomes after bootstrapping.</p></div><div><h3>Results</h3><p>The modelled 2-year OS rate of cCRT-ICB reached 71 % (95 % confidence intervals, CI 62 %, 84 %) and 66 % (95 % CI: 53 %, 81 %) for stage IIIA and IIIB/C, respectively, given 60 Gy in 2 Gy-per-fraction. 60 Gy in 30 fractions remained the best schedule for cCRT-ICB, whereas modest dose de-escalation to 55 Gy only reduced the OS in 2 %. Sequential CRT (sCRT)-ICB provided 6 % OS increases versus the best OS rate achieved by sCRT alone. Photon MHD-sparing achieved a 5–10 % increase in modelled 2-year OS, with protons providing a further roughly 5–10 % increase.</p></div><div><h3>Conclusion</h3><p>Neither dose-escalation nor de-escalation relative to 60 Gy in 30 fractions influenced the survival with cCRT-ICB, while 5 Gy dose de-escalation might benefit patients with heavily irradiated organs at risk. Cardiac-sparing improved OS, and protons provided advantages for tumours anatomically overlapped or lay below the heart.</p></div>","PeriodicalId":21041,"journal":{"name":"Radiotherapy and Oncology","volume":"200 ","pages":"Article 110477"},"PeriodicalIF":5.3000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Parallel explorations in LA-NSCLC: Chemoradiation dose-response optimisation considering immunotherapy and cardiac toxicity sparing\",\"authors\":\"Huei-Tyng Huang\",\"doi\":\"10.1016/j.radonc.2024.110477\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background and purpose</h3><p>Chemoradiotherapy (CRT) for locally-advanced non-small cell lung cancer (LA-NSCLC) has undergone advances, including increased overall survival (OS) when combined with immune checkpoint blockade (ICB), and using cardiac-sparing techniques to reduce the radiotoxicity. This research investigated 1) how radiotherapy schedules can be optimised with CRT-ICB schemes, and 2) how cardiac-sparing might change the OS for concurrent CRT (cCRT).</p></div><div><h3>Methods and materials</h3><p>Survival data and dosimetric indices were sourced from published studies, with 2-year OS standardised and the hazard ratio of mean heart dose (MHD) against radiotoxicity tabulated in purpose. A published CRT dose–response model was selected, then modified with ICB and cardiac-sparing hypotheses. Models were maximum likelihood fitted, then visualised the prediction outcomes after bootstrapping.</p></div><div><h3>Results</h3><p>The modelled 2-year OS rate of cCRT-ICB reached 71 % (95 % confidence intervals, CI 62 %, 84 %) and 66 % (95 % CI: 53 %, 81 %) for stage IIIA and IIIB/C, respectively, given 60 Gy in 2 Gy-per-fraction. 60 Gy in 30 fractions remained the best schedule for cCRT-ICB, whereas modest dose de-escalation to 55 Gy only reduced the OS in 2 %. Sequential CRT (sCRT)-ICB provided 6 % OS increases versus the best OS rate achieved by sCRT alone. Photon MHD-sparing achieved a 5–10 % increase in modelled 2-year OS, with protons providing a further roughly 5–10 % increase.</p></div><div><h3>Conclusion</h3><p>Neither dose-escalation nor de-escalation relative to 60 Gy in 30 fractions influenced the survival with cCRT-ICB, while 5 Gy dose de-escalation might benefit patients with heavily irradiated organs at risk. Cardiac-sparing improved OS, and protons provided advantages for tumours anatomically overlapped or lay below the heart.</p></div>\",\"PeriodicalId\":21041,\"journal\":{\"name\":\"Radiotherapy and Oncology\",\"volume\":\"200 \",\"pages\":\"Article 110477\"},\"PeriodicalIF\":5.3000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiotherapy and Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0167814024007473\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiotherapy and Oncology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0167814024007473","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/15 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Parallel explorations in LA-NSCLC: Chemoradiation dose-response optimisation considering immunotherapy and cardiac toxicity sparing
Background and purpose
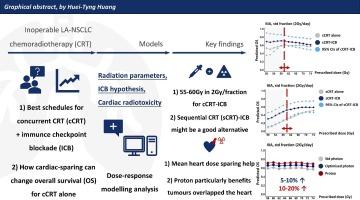
Chemoradiotherapy (CRT) for locally-advanced non-small cell lung cancer (LA-NSCLC) has undergone advances, including increased overall survival (OS) when combined with immune checkpoint blockade (ICB), and using cardiac-sparing techniques to reduce the radiotoxicity. This research investigated 1) how radiotherapy schedules can be optimised with CRT-ICB schemes, and 2) how cardiac-sparing might change the OS for concurrent CRT (cCRT).
Methods and materials
Survival data and dosimetric indices were sourced from published studies, with 2-year OS standardised and the hazard ratio of mean heart dose (MHD) against radiotoxicity tabulated in purpose. A published CRT dose–response model was selected, then modified with ICB and cardiac-sparing hypotheses. Models were maximum likelihood fitted, then visualised the prediction outcomes after bootstrapping.
Results
The modelled 2-year OS rate of cCRT-ICB reached 71 % (95 % confidence intervals, CI 62 %, 84 %) and 66 % (95 % CI: 53 %, 81 %) for stage IIIA and IIIB/C, respectively, given 60 Gy in 2 Gy-per-fraction. 60 Gy in 30 fractions remained the best schedule for cCRT-ICB, whereas modest dose de-escalation to 55 Gy only reduced the OS in 2 %. Sequential CRT (sCRT)-ICB provided 6 % OS increases versus the best OS rate achieved by sCRT alone. Photon MHD-sparing achieved a 5–10 % increase in modelled 2-year OS, with protons providing a further roughly 5–10 % increase.
Conclusion
Neither dose-escalation nor de-escalation relative to 60 Gy in 30 fractions influenced the survival with cCRT-ICB, while 5 Gy dose de-escalation might benefit patients with heavily irradiated organs at risk. Cardiac-sparing improved OS, and protons provided advantages for tumours anatomically overlapped or lay below the heart.
期刊介绍:
Radiotherapy and Oncology publishes papers describing original research as well as review articles. It covers areas of interest relating to radiation oncology. This includes: clinical radiotherapy, combined modality treatment, translational studies, epidemiological outcomes, imaging, dosimetry, and radiation therapy planning, experimental work in radiobiology, chemobiology, hyperthermia and tumour biology, as well as data science in radiation oncology and physics aspects relevant to oncology.Papers on more general aspects of interest to the radiation oncologist including chemotherapy, surgery and immunology are also published.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
