Marta Adam, Dora Arhanić, Iva Z Alajbeg, Grgur Matolić, Sonja Krofak, Ema Vrbanović Đuričić
{"title":"预防气管插管过程中的口腔损伤:患者和麻醉师的观点。","authors":"Marta Adam, Dora Arhanić, Iva Z Alajbeg, Grgur Matolić, Sonja Krofak, Ema Vrbanović Đuričić","doi":"10.5644/ama2006-124.445","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim was to design accessible, simple, inexpensive protection for teeth and soft tissues during ETI, compare damage occurrence with and without protection, and investigate post-ETI orofacial pain symptoms.</p><p><strong>Materials and methods: </strong>The selection procedure for adequate protection was carried out after which a reduced elastomer mouthguard was selected. Fifty patients were divided into 2 groups. In the first group, ETI was carried out using a mouthguard, while in the second group it was performed without it. The mouthguard was fabricated by anesthesiologists. After the ETI procedure, the patients and anesthesiologists were asked to complete a survey.</p><p><strong>Results: </strong>No difference in intubation severity and time required for intubation between the two groups was present. Seven patients from the non-mouthguard group suffered injuries during the ETI procedure. No injuries were present in the mouthguard group. In 92% of cases anesthesiologists agreed that mouthguards should be used during ETI. However, most of them (96% of cases) agree that the mouthguard should be used only when there is an increased risk of tooth loss and/or tooth damage. There was a significant ETI effect on the emergence of new orofacial pain cases.</p><p><strong>Conclusion: </strong>The mouthguard adequately protected dental and soft tissues and did not affect the work of the anesthesiologist. A significantly higher number of patients experiencing temporomandibular joint and masticatory muscles pain after surgery indicates that ETI might be a risk factor for orofacial pain.</p>","PeriodicalId":38313,"journal":{"name":"Acta medica academica","volume":" ","pages":"123-135"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11626239/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prevention of Oral Injuries during Endotracheal Intubation: Patients' and Anesthesiologists' Perspective.\",\"authors\":\"Marta Adam, Dora Arhanić, Iva Z Alajbeg, Grgur Matolić, Sonja Krofak, Ema Vrbanović Đuričić\",\"doi\":\"10.5644/ama2006-124.445\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The aim was to design accessible, simple, inexpensive protection for teeth and soft tissues during ETI, compare damage occurrence with and without protection, and investigate post-ETI orofacial pain symptoms.</p><p><strong>Materials and methods: </strong>The selection procedure for adequate protection was carried out after which a reduced elastomer mouthguard was selected. Fifty patients were divided into 2 groups. In the first group, ETI was carried out using a mouthguard, while in the second group it was performed without it. The mouthguard was fabricated by anesthesiologists. After the ETI procedure, the patients and anesthesiologists were asked to complete a survey.</p><p><strong>Results: </strong>No difference in intubation severity and time required for intubation between the two groups was present. Seven patients from the non-mouthguard group suffered injuries during the ETI procedure. No injuries were present in the mouthguard group. In 92% of cases anesthesiologists agreed that mouthguards should be used during ETI. However, most of them (96% of cases) agree that the mouthguard should be used only when there is an increased risk of tooth loss and/or tooth damage. There was a significant ETI effect on the emergence of new orofacial pain cases.</p><p><strong>Conclusion: </strong>The mouthguard adequately protected dental and soft tissues and did not affect the work of the anesthesiologist. A significantly higher number of patients experiencing temporomandibular joint and masticatory muscles pain after surgery indicates that ETI might be a risk factor for orofacial pain.</p>\",\"PeriodicalId\":38313,\"journal\":{\"name\":\"Acta medica academica\",\"volume\":\" \",\"pages\":\"123-135\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11626239/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta medica academica\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5644/ama2006-124.445\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta medica academica","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5644/ama2006-124.445","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
目的:旨在为 ETI 期间的牙齿和软组织设计简单、廉价的保护装置:目的是为 ETI 期间的牙齿和软组织设计方便、简单、廉价的保护装置,比较有保护装置和无保护装置时的损伤发生情况,并调查 ETI 后的口面部疼痛症状:材料: 对适当的保护措施进行了选择,然后选择了一种缩小的弹性体护齿。50 名患者分为两组。第一组使用护齿进行 ETI,第二组不使用护齿。护齿由麻醉师制作。ETI 过程结束后,患者和麻醉师被要求填写一份调查问卷:结果:两组患者的插管严重程度和插管所需时间没有差异。在 ETI 过程中,无护齿组有七名患者受伤。护齿组没有受伤。在 92% 的病例中,麻醉师同意在 ETI 过程中使用护齿。不过,他们中的大多数(96%)都认为,只有在牙齿脱落和/或牙齿损坏的风险增加时才应使用护齿器。结论:ETI 对新出现的口面部疼痛病例有明显的影响:护齿器可充分保护牙齿和软组织,不会影响麻醉师的工作。手术后出现颞下颌关节和咀嚼肌疼痛的患者人数明显增多,这表明 ETI 可能是导致口面部疼痛的一个危险因素。
Prevention of Oral Injuries during Endotracheal Intubation: Patients' and Anesthesiologists' Perspective.
Objective: The aim was to design accessible, simple, inexpensive protection for teeth and soft tissues during ETI, compare damage occurrence with and without protection, and investigate post-ETI orofacial pain symptoms.
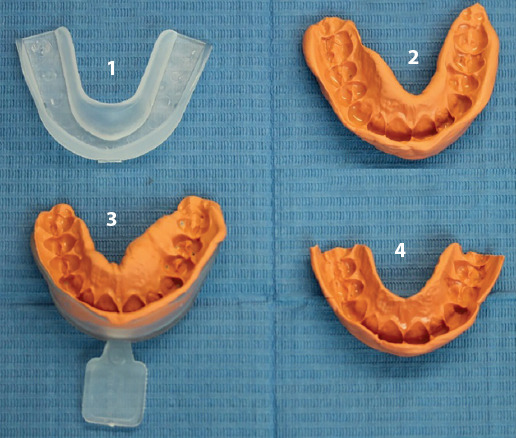
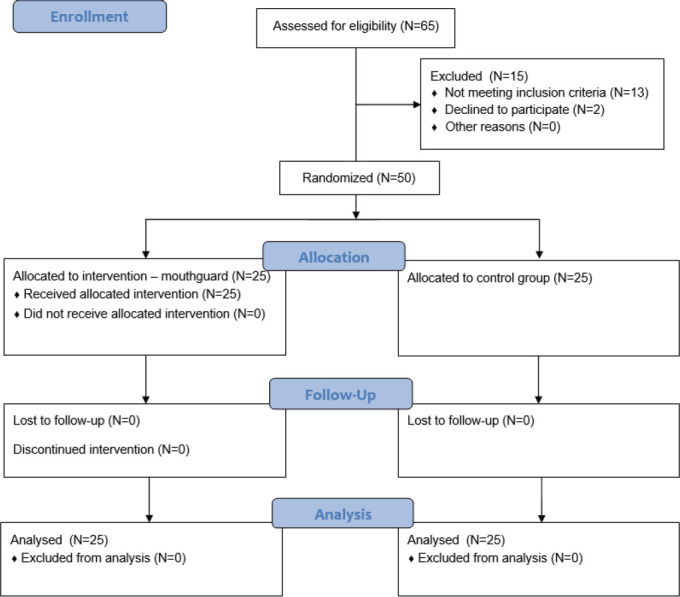
Materials and methods: The selection procedure for adequate protection was carried out after which a reduced elastomer mouthguard was selected. Fifty patients were divided into 2 groups. In the first group, ETI was carried out using a mouthguard, while in the second group it was performed without it. The mouthguard was fabricated by anesthesiologists. After the ETI procedure, the patients and anesthesiologists were asked to complete a survey.
Results: No difference in intubation severity and time required for intubation between the two groups was present. Seven patients from the non-mouthguard group suffered injuries during the ETI procedure. No injuries were present in the mouthguard group. In 92% of cases anesthesiologists agreed that mouthguards should be used during ETI. However, most of them (96% of cases) agree that the mouthguard should be used only when there is an increased risk of tooth loss and/or tooth damage. There was a significant ETI effect on the emergence of new orofacial pain cases.
Conclusion: The mouthguard adequately protected dental and soft tissues and did not affect the work of the anesthesiologist. A significantly higher number of patients experiencing temporomandibular joint and masticatory muscles pain after surgery indicates that ETI might be a risk factor for orofacial pain.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
