Jane S. Saczynski PhD, Benjamin Koethe MPH, Donna Marie Fick PhD, Quynh T. Vo MPH, John W. Devlin PharmD, Edward R. Marcantonio MD, Becky A. Briesacher PhD
{"title":"专业护理机构中的认知和功能变化:谵妄和阿尔茨海默病及相关痴呆症的差异。","authors":"Jane S. Saczynski PhD, Benjamin Koethe MPH, Donna Marie Fick PhD, Quynh T. Vo MPH, John W. Devlin PharmD, Edward R. Marcantonio MD, Becky A. Briesacher PhD","doi":"10.1111/jgs.19112","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Whether cognitive and functional recovery in skilled nursing facilities (SNF) following hospitalization differs by delirium and Alzheimer's disease related dementias (ADRD) has not been examined.</p>\n </section>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>To compare change in cognition and function among short-stay SNF patients with delirium, ADRD, or both.</p>\n </section>\n \n <section>\n \n <h3> Design</h3>\n \n <p>Retrospective cohort study using claims data from 2011 to 2013.</p>\n </section>\n \n <section>\n \n <h3> Setting</h3>\n \n <p>Centers for Medicare and Medicaid certified SNFs.</p>\n </section>\n \n <section>\n \n <h3> Participants</h3>\n \n <p>A total of 740,838 older adults newly admitted to a short-stay SNF without prevalent ADRD who had at least two assessments of cognition and function.</p>\n </section>\n \n <section>\n \n <h3> Measurements</h3>\n \n <p>Incident delirium was measured by the Minimum Data Set (MDS) Confusion Assessment Method and ICD-9 codes, and incident ADRD by ICD-9 codes and MDS diagnoses. Cognitive improvement was a better or maximum score on the MDS Brief Interview for Mental Status, and functional recovery was a better or maximum score on the MDS Activities of Daily Living Scale.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Within 30 days of SNF admission, the rate of cognitive improvement in patients with both delirium/ADRD was half that of patients with neither delirium/ADRD (HR = 0.45, 95% CI:0.43, 0.46). The ADRD-only and delirium-only groups also were 43% less likely to have improved cognition or function compared to those with neither delirium/ADRD (HR = 0.57, 95% CI:0.56, 0.58 and HR = 0.57, 95% CI:0.55, 0.60, respectively). Functional improvement was less likely in patients with both delirium/ADRD, as well (HR = 0.85, 95% CI:0.83, 0.87). The ADRD only and delirium only groups were also less likely to improve in function (HR = 0.93, 95% CI:0.92, 0.94 and HR = 0.92, 95% CI:0.90, 0.93, respectively) compared to those with neither delirium/ADRD.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Among older adults without dementia admitted to SNF for post-acute care following hospitalization, a positive screen for delirium and a new diagnosis of ADRD, within 7 days of SNF admission, were both significantly associated with worse cognitive and functional recovery. Patients with both delirium and new ADRD had the worst cognitive and functional recovery.</p>\n </section>\n </div>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 11","pages":"3501-3509"},"PeriodicalIF":4.5000,"publicationDate":"2024-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19112","citationCount":"0","resultStr":"{\"title\":\"Cognitive and functional change in skilled nursing facilities: Differences by delirium and Alzheimer's disease and related dementias\",\"authors\":\"Jane S. Saczynski PhD, Benjamin Koethe MPH, Donna Marie Fick PhD, Quynh T. Vo MPH, John W. Devlin PharmD, Edward R. Marcantonio MD, Becky A. Briesacher PhD\",\"doi\":\"10.1111/jgs.19112\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Whether cognitive and functional recovery in skilled nursing facilities (SNF) following hospitalization differs by delirium and Alzheimer's disease related dementias (ADRD) has not been examined.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>To compare change in cognition and function among short-stay SNF patients with delirium, ADRD, or both.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Design</h3>\\n \\n <p>Retrospective cohort study using claims data from 2011 to 2013.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Setting</h3>\\n \\n <p>Centers for Medicare and Medicaid certified SNFs.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Participants</h3>\\n \\n <p>A total of 740,838 older adults newly admitted to a short-stay SNF without prevalent ADRD who had at least two assessments of cognition and function.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Measurements</h3>\\n \\n <p>Incident delirium was measured by the Minimum Data Set (MDS) Confusion Assessment Method and ICD-9 codes, and incident ADRD by ICD-9 codes and MDS diagnoses. Cognitive improvement was a better or maximum score on the MDS Brief Interview for Mental Status, and functional recovery was a better or maximum score on the MDS Activities of Daily Living Scale.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Within 30 days of SNF admission, the rate of cognitive improvement in patients with both delirium/ADRD was half that of patients with neither delirium/ADRD (HR = 0.45, 95% CI:0.43, 0.46). The ADRD-only and delirium-only groups also were 43% less likely to have improved cognition or function compared to those with neither delirium/ADRD (HR = 0.57, 95% CI:0.56, 0.58 and HR = 0.57, 95% CI:0.55, 0.60, respectively). Functional improvement was less likely in patients with both delirium/ADRD, as well (HR = 0.85, 95% CI:0.83, 0.87). The ADRD only and delirium only groups were also less likely to improve in function (HR = 0.93, 95% CI:0.92, 0.94 and HR = 0.92, 95% CI:0.90, 0.93, respectively) compared to those with neither delirium/ADRD.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Among older adults without dementia admitted to SNF for post-acute care following hospitalization, a positive screen for delirium and a new diagnosis of ADRD, within 7 days of SNF admission, were both significantly associated with worse cognitive and functional recovery. Patients with both delirium and new ADRD had the worst cognitive and functional recovery.</p>\\n </section>\\n </div>\",\"PeriodicalId\":17240,\"journal\":{\"name\":\"Journal of the American Geriatrics Society\",\"volume\":\"72 11\",\"pages\":\"3501-3509\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2024-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19112\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Geriatrics Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19112\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19112","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
Cognitive and functional change in skilled nursing facilities: Differences by delirium and Alzheimer's disease and related dementias
Background
Whether cognitive and functional recovery in skilled nursing facilities (SNF) following hospitalization differs by delirium and Alzheimer's disease related dementias (ADRD) has not been examined.
Objective
To compare change in cognition and function among short-stay SNF patients with delirium, ADRD, or both.
Design
Retrospective cohort study using claims data from 2011 to 2013.
Setting
Centers for Medicare and Medicaid certified SNFs.
Participants
A total of 740,838 older adults newly admitted to a short-stay SNF without prevalent ADRD who had at least two assessments of cognition and function.
Measurements
Incident delirium was measured by the Minimum Data Set (MDS) Confusion Assessment Method and ICD-9 codes, and incident ADRD by ICD-9 codes and MDS diagnoses. Cognitive improvement was a better or maximum score on the MDS Brief Interview for Mental Status, and functional recovery was a better or maximum score on the MDS Activities of Daily Living Scale.
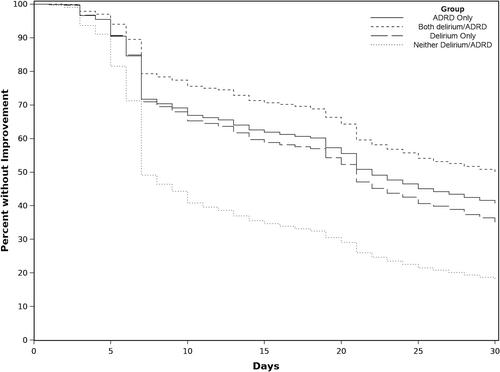
Results
Within 30 days of SNF admission, the rate of cognitive improvement in patients with both delirium/ADRD was half that of patients with neither delirium/ADRD (HR = 0.45, 95% CI:0.43, 0.46). The ADRD-only and delirium-only groups also were 43% less likely to have improved cognition or function compared to those with neither delirium/ADRD (HR = 0.57, 95% CI:0.56, 0.58 and HR = 0.57, 95% CI:0.55, 0.60, respectively). Functional improvement was less likely in patients with both delirium/ADRD, as well (HR = 0.85, 95% CI:0.83, 0.87). The ADRD only and delirium only groups were also less likely to improve in function (HR = 0.93, 95% CI:0.92, 0.94 and HR = 0.92, 95% CI:0.90, 0.93, respectively) compared to those with neither delirium/ADRD.
Conclusions
Among older adults without dementia admitted to SNF for post-acute care following hospitalization, a positive screen for delirium and a new diagnosis of ADRD, within 7 days of SNF admission, were both significantly associated with worse cognitive and functional recovery. Patients with both delirium and new ADRD had the worst cognitive and functional recovery.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
