{"title":"使用废透析液和 Kt/Vurea 方程比较血液透析尿素清除率。","authors":"Priyanka Khatri, Andrew Davenport","doi":"10.1111/aor.14848","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Dialysis adequacy is traditionally calculated from pre- and post-hemodialysis session serum urea concentrations and expressed as the urea reduction ratio, or Kt/Vurea. However, with increasing hemodiafiltration usage, we wished to determine whether there were any differences between standard Kt/Vurea equations and directly measured spent dialysate urea clearance.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Urea clearance was measured from collected effluent dialysate and compared with various other methods of Kt/Vurea calculation, including change in total body urea from measuring pre- and post-total body water with bioimpedance and the Watson equation, by standard Kt/V equations, and online clearance measurements using effective ionic dialysance (OLC).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We compared urea clearance in 41 patients, 56.1% male, mean age 69.3 ± 12.6 years with 87.8% treated by hemodiafiltration. Reduction in total body urea was greater when estimating changes in total body urea, compared to measured dialysate losses of 58.4% (48.5–67.6) vs 71.6% (62.1–78), <i>p</i> < 0.01. Sessional urea clearance (Kt/Vurea) was greater using the online Solute-Solver program compared to OLC, median 1.45(1.13–1.75) vs 1.2 (0.93–1.4), and 2nd generation Kt/V equations 1.3 (1.02–1.66), <i>p</i> < 0.01, but not different from estimated total body urea clearance 1.36 (1.15–1.73) and dialysate clearance 1.36 (1.07–1.76). The mean bias compared to the Solute-Solver program was greatest with OLC (−0.25), compared to second-generation equations (−0.02), estimated total body clearance (−0.02) and measured dialysate clearance (−0.01).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>This study demonstrated that the result from equations estimating urea clearance indirectly from pre- and postblood samples from hemo- and hemodiafiltration treatments was highly correlated with direct measurements of dialysate urea clearance.</p>\n </section>\n </div>","PeriodicalId":8450,"journal":{"name":"Artificial organs","volume":"49 1","pages":"85-92"},"PeriodicalIF":2.3000,"publicationDate":"2024-08-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11687206/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of hemodialysis urea clearance using spent dialysate and Kt/Vurea equations\",\"authors\":\"Priyanka Khatri, Andrew Davenport\",\"doi\":\"10.1111/aor.14848\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>Dialysis adequacy is traditionally calculated from pre- and post-hemodialysis session serum urea concentrations and expressed as the urea reduction ratio, or Kt/Vurea. However, with increasing hemodiafiltration usage, we wished to determine whether there were any differences between standard Kt/Vurea equations and directly measured spent dialysate urea clearance.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Urea clearance was measured from collected effluent dialysate and compared with various other methods of Kt/Vurea calculation, including change in total body urea from measuring pre- and post-total body water with bioimpedance and the Watson equation, by standard Kt/V equations, and online clearance measurements using effective ionic dialysance (OLC).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We compared urea clearance in 41 patients, 56.1% male, mean age 69.3 ± 12.6 years with 87.8% treated by hemodiafiltration. Reduction in total body urea was greater when estimating changes in total body urea, compared to measured dialysate losses of 58.4% (48.5–67.6) vs 71.6% (62.1–78), <i>p</i> < 0.01. Sessional urea clearance (Kt/Vurea) was greater using the online Solute-Solver program compared to OLC, median 1.45(1.13–1.75) vs 1.2 (0.93–1.4), and 2nd generation Kt/V equations 1.3 (1.02–1.66), <i>p</i> < 0.01, but not different from estimated total body urea clearance 1.36 (1.15–1.73) and dialysate clearance 1.36 (1.07–1.76). The mean bias compared to the Solute-Solver program was greatest with OLC (−0.25), compared to second-generation equations (−0.02), estimated total body clearance (−0.02) and measured dialysate clearance (−0.01).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>This study demonstrated that the result from equations estimating urea clearance indirectly from pre- and postblood samples from hemo- and hemodiafiltration treatments was highly correlated with direct measurements of dialysate urea clearance.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8450,\"journal\":{\"name\":\"Artificial organs\",\"volume\":\"49 1\",\"pages\":\"85-92\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-08-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11687206/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Artificial organs\",\"FirstCategoryId\":\"5\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/aor.14848\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENGINEERING, BIOMEDICAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Artificial organs","FirstCategoryId":"5","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/aor.14848","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
Comparison of hemodialysis urea clearance using spent dialysate and Kt/Vurea equations
Introduction
Dialysis adequacy is traditionally calculated from pre- and post-hemodialysis session serum urea concentrations and expressed as the urea reduction ratio, or Kt/Vurea. However, with increasing hemodiafiltration usage, we wished to determine whether there were any differences between standard Kt/Vurea equations and directly measured spent dialysate urea clearance.
Methods
Urea clearance was measured from collected effluent dialysate and compared with various other methods of Kt/Vurea calculation, including change in total body urea from measuring pre- and post-total body water with bioimpedance and the Watson equation, by standard Kt/V equations, and online clearance measurements using effective ionic dialysance (OLC).
Results
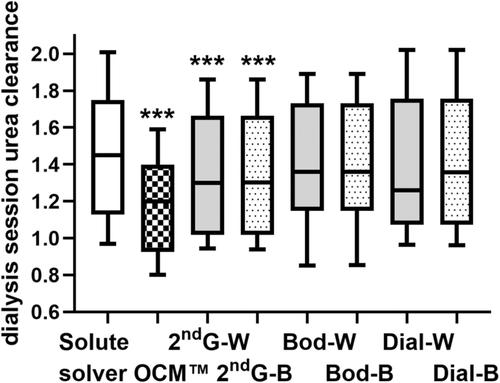
We compared urea clearance in 41 patients, 56.1% male, mean age 69.3 ± 12.6 years with 87.8% treated by hemodiafiltration. Reduction in total body urea was greater when estimating changes in total body urea, compared to measured dialysate losses of 58.4% (48.5–67.6) vs 71.6% (62.1–78), p < 0.01. Sessional urea clearance (Kt/Vurea) was greater using the online Solute-Solver program compared to OLC, median 1.45(1.13–1.75) vs 1.2 (0.93–1.4), and 2nd generation Kt/V equations 1.3 (1.02–1.66), p < 0.01, but not different from estimated total body urea clearance 1.36 (1.15–1.73) and dialysate clearance 1.36 (1.07–1.76). The mean bias compared to the Solute-Solver program was greatest with OLC (−0.25), compared to second-generation equations (−0.02), estimated total body clearance (−0.02) and measured dialysate clearance (−0.01).
Conclusion
This study demonstrated that the result from equations estimating urea clearance indirectly from pre- and postblood samples from hemo- and hemodiafiltration treatments was highly correlated with direct measurements of dialysate urea clearance.
期刊介绍:
Artificial Organs is the official peer reviewed journal of The International Federation for Artificial Organs (Members of the Federation are: The American Society for Artificial Internal Organs, The European Society for Artificial Organs, and The Japanese Society for Artificial Organs), The International Faculty for Artificial Organs, the International Society for Rotary Blood Pumps, The International Society for Pediatric Mechanical Cardiopulmonary Support, and the Vienna International Workshop on Functional Electrical Stimulation. Artificial Organs publishes original research articles dealing with developments in artificial organs applications and treatment modalities and their clinical applications worldwide. Membership in the Societies listed above is not a prerequisite for publication. Articles are published without charge to the author except for color figures and excess page charges as noted.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
