{"title":"FAST-ED 评估急诊科急性缺血性脑卒中大血管闭塞的准确性。","authors":"Chatchanan Pornpanit, Punnaporn Loymai, Nattaphol Uransilp, Winchana Srivilaithon","doi":"10.2147/OAEM.S461177","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute large vessel occlusion stroke (LVOS) requires swift and precise assessment for effective treatment. The Field Assessment Stroke Triage for Emergency Destination (FAST-ED) protocol shows promise for rapid LVOS evaluation but lacks extensive validation. This study aims to assess the accuracy of FAST-ED in predicting LVOS and compare its predictive capability with the National Institute of Health Stroke Scale (NIHSS).</p><p><strong>Methods: </strong>This prospective cross-sectional study was conducted at Thammasat University Hospital. Participants included those aged 18 years or older who presented with symptoms of acute stroke syndrome within 24 hours of onset. The study focused on comparing FAST-ED assessments by emergency department physicians with NIHSS evaluations by neurologists, followed by vascular imaging, which included brain multiphase CT angiography, MRI with MRA, and transcranial Doppler ultrasound combined with carotid Doppler ultrasound. Statistical analyses included the use of AuROC to assess the effectiveness of FAST-ED and to compare FAST-ED with NIHSS.</p><p><strong>Results: </strong>130 patients were included in the analysis, with 47 diagnosed with LVOS. No significant differences were found in most baseline characteristics between LVOS and non-LVOS groups, except for a higher prevalence of atrial fibrillation and lower systolic blood pressure in the LVOS group. The FAST-ED scale demonstrated a fair ability to predict LVOS with an AuROC of 0.79 (95% confidence interval (CI); 0.70, 0.87). A FAST-ED cut point of ≥4 showed improved specificity and likelihood ratio. Comparing FAST-ED≥4 with NIHSS≥6 revealed similar AuROC (0.74, 95% CI; 0.65, 0.82 and 0.72, 95% CI; 0.64, 0.80, respectively), with no significant statistical difference (p=0.661).</p><p><strong>Conclusion: </strong>FAST-ED scale, especially with a cut-off point of ≥4, exhibits fair overall accuracy in predicting LVOS in patients who presented with suspected acute stroke within 24 hours at the ED. This predictive capability is closely comparable to that of the NIHSS at a cut-off point of ≥6.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"16 ","pages":"203-210"},"PeriodicalIF":1.5000,"publicationDate":"2024-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11346489/pdf/","citationCount":"0","resultStr":"{\"title\":\"Accuracy of FAST-ED for Assessment Large Vessel Occlusion of Acute Ischemic Stroke in Emergency Department.\",\"authors\":\"Chatchanan Pornpanit, Punnaporn Loymai, Nattaphol Uransilp, Winchana Srivilaithon\",\"doi\":\"10.2147/OAEM.S461177\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute large vessel occlusion stroke (LVOS) requires swift and precise assessment for effective treatment. The Field Assessment Stroke Triage for Emergency Destination (FAST-ED) protocol shows promise for rapid LVOS evaluation but lacks extensive validation. This study aims to assess the accuracy of FAST-ED in predicting LVOS and compare its predictive capability with the National Institute of Health Stroke Scale (NIHSS).</p><p><strong>Methods: </strong>This prospective cross-sectional study was conducted at Thammasat University Hospital. Participants included those aged 18 years or older who presented with symptoms of acute stroke syndrome within 24 hours of onset. The study focused on comparing FAST-ED assessments by emergency department physicians with NIHSS evaluations by neurologists, followed by vascular imaging, which included brain multiphase CT angiography, MRI with MRA, and transcranial Doppler ultrasound combined with carotid Doppler ultrasound. Statistical analyses included the use of AuROC to assess the effectiveness of FAST-ED and to compare FAST-ED with NIHSS.</p><p><strong>Results: </strong>130 patients were included in the analysis, with 47 diagnosed with LVOS. No significant differences were found in most baseline characteristics between LVOS and non-LVOS groups, except for a higher prevalence of atrial fibrillation and lower systolic blood pressure in the LVOS group. The FAST-ED scale demonstrated a fair ability to predict LVOS with an AuROC of 0.79 (95% confidence interval (CI); 0.70, 0.87). A FAST-ED cut point of ≥4 showed improved specificity and likelihood ratio. Comparing FAST-ED≥4 with NIHSS≥6 revealed similar AuROC (0.74, 95% CI; 0.65, 0.82 and 0.72, 95% CI; 0.64, 0.80, respectively), with no significant statistical difference (p=0.661).</p><p><strong>Conclusion: </strong>FAST-ED scale, especially with a cut-off point of ≥4, exhibits fair overall accuracy in predicting LVOS in patients who presented with suspected acute stroke within 24 hours at the ED. This predictive capability is closely comparable to that of the NIHSS at a cut-off point of ≥6.</p>\",\"PeriodicalId\":45096,\"journal\":{\"name\":\"Open Access Emergency Medicine\",\"volume\":\"16 \",\"pages\":\"203-210\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11346489/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S461177\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S461177","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Accuracy of FAST-ED for Assessment Large Vessel Occlusion of Acute Ischemic Stroke in Emergency Department.
Background: Acute large vessel occlusion stroke (LVOS) requires swift and precise assessment for effective treatment. The Field Assessment Stroke Triage for Emergency Destination (FAST-ED) protocol shows promise for rapid LVOS evaluation but lacks extensive validation. This study aims to assess the accuracy of FAST-ED in predicting LVOS and compare its predictive capability with the National Institute of Health Stroke Scale (NIHSS).
Methods: This prospective cross-sectional study was conducted at Thammasat University Hospital. Participants included those aged 18 years or older who presented with symptoms of acute stroke syndrome within 24 hours of onset. The study focused on comparing FAST-ED assessments by emergency department physicians with NIHSS evaluations by neurologists, followed by vascular imaging, which included brain multiphase CT angiography, MRI with MRA, and transcranial Doppler ultrasound combined with carotid Doppler ultrasound. Statistical analyses included the use of AuROC to assess the effectiveness of FAST-ED and to compare FAST-ED with NIHSS.
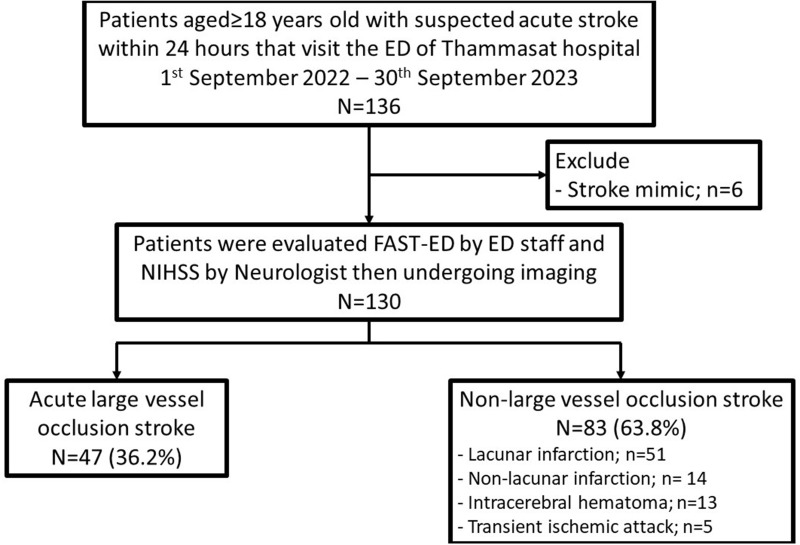
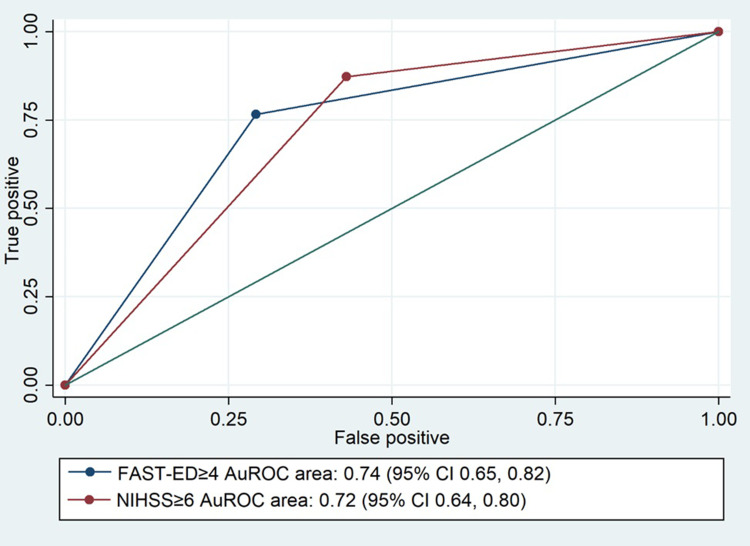
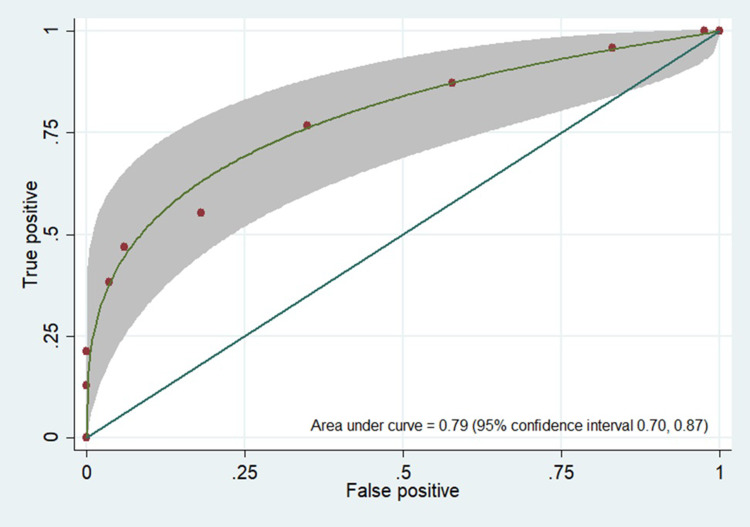
Results: 130 patients were included in the analysis, with 47 diagnosed with LVOS. No significant differences were found in most baseline characteristics between LVOS and non-LVOS groups, except for a higher prevalence of atrial fibrillation and lower systolic blood pressure in the LVOS group. The FAST-ED scale demonstrated a fair ability to predict LVOS with an AuROC of 0.79 (95% confidence interval (CI); 0.70, 0.87). A FAST-ED cut point of ≥4 showed improved specificity and likelihood ratio. Comparing FAST-ED≥4 with NIHSS≥6 revealed similar AuROC (0.74, 95% CI; 0.65, 0.82 and 0.72, 95% CI; 0.64, 0.80, respectively), with no significant statistical difference (p=0.661).
Conclusion: FAST-ED scale, especially with a cut-off point of ≥4, exhibits fair overall accuracy in predicting LVOS in patients who presented with suspected acute stroke within 24 hours at the ED. This predictive capability is closely comparable to that of the NIHSS at a cut-off point of ≥6.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
