Janeni Jeevanathan , Sigrid M. Blom , Thomas Olsen , Kirsten B. Holven , Erik K. Arnesen , Torleif Trydal , Børge G. Nordestgaard , Michael Sovershaev , Ying Chen , Kjetil Retterstøl , Jacob J. Christensen
{"title":"在临床环境中从一种脂蛋白(a)检测方法过渡到另一种检测方法的实际影响","authors":"Janeni Jeevanathan , Sigrid M. Blom , Thomas Olsen , Kirsten B. Holven , Erik K. Arnesen , Torleif Trydal , Børge G. Nordestgaard , Michael Sovershaev , Ying Chen , Kjetil Retterstøl , Jacob J. Christensen","doi":"10.1016/j.ajpc.2024.100726","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and aims</h3><p>Different lipoprotein(a) [Lp(a)] assays may affect risk stratification of individuals and thus clinical decision-making. We aimed to investigate how transitioning between Lp(a) assays at a large central laboratory affected the proportion of individuals with Lp(a) result above clinical thresholds.</p></div><div><h3>Methods</h3><p>We studied nationwide clinical laboratory data including 185,493 unique individuals (47.7 % women) aged 18-50 years with 272,463 Lp(a) measurements using Roche (2000-2009) and Siemens Lp(a) assay (2009-2019).</p></div><div><h3>Results</h3><p>While the majority of individuals (66-75 %) had low levels of Lp(a) (<30 mg/dL) independent of the assay used, the Roche assay detected 20 % more individuals with Lp(a) >50 mg/dL, 40 % more individuals with Lp(a) >100 mg/dL and 80 % more individuals with Lp(a) > 180 mg/dL than the currently used Siemens assay, likely due to calibration differences.</p></div><div><h3>Conclusion</h3><p>Transitioning from one Lp(a) immunoassay to another had significant impact on Lp(a) results, particularly in individuals approaching clinically relevant Lp(a) thresholds.</p></div>","PeriodicalId":72173,"journal":{"name":"American journal of preventive cardiology","volume":"19 ","pages":"Article 100726"},"PeriodicalIF":5.4000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2666667724000941/pdfft?md5=b4e82c85b1837ad5e8bce9d75dcc8758&pid=1-s2.0-S2666667724000941-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Real-world impact of transitioning from one lipoprotein(a) assay to another in a clinical setting\",\"authors\":\"Janeni Jeevanathan , Sigrid M. Blom , Thomas Olsen , Kirsten B. Holven , Erik K. Arnesen , Torleif Trydal , Børge G. Nordestgaard , Michael Sovershaev , Ying Chen , Kjetil Retterstøl , Jacob J. Christensen\",\"doi\":\"10.1016/j.ajpc.2024.100726\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background and aims</h3><p>Different lipoprotein(a) [Lp(a)] assays may affect risk stratification of individuals and thus clinical decision-making. We aimed to investigate how transitioning between Lp(a) assays at a large central laboratory affected the proportion of individuals with Lp(a) result above clinical thresholds.</p></div><div><h3>Methods</h3><p>We studied nationwide clinical laboratory data including 185,493 unique individuals (47.7 % women) aged 18-50 years with 272,463 Lp(a) measurements using Roche (2000-2009) and Siemens Lp(a) assay (2009-2019).</p></div><div><h3>Results</h3><p>While the majority of individuals (66-75 %) had low levels of Lp(a) (<30 mg/dL) independent of the assay used, the Roche assay detected 20 % more individuals with Lp(a) >50 mg/dL, 40 % more individuals with Lp(a) >100 mg/dL and 80 % more individuals with Lp(a) > 180 mg/dL than the currently used Siemens assay, likely due to calibration differences.</p></div><div><h3>Conclusion</h3><p>Transitioning from one Lp(a) immunoassay to another had significant impact on Lp(a) results, particularly in individuals approaching clinically relevant Lp(a) thresholds.</p></div>\",\"PeriodicalId\":72173,\"journal\":{\"name\":\"American journal of preventive cardiology\",\"volume\":\"19 \",\"pages\":\"Article 100726\"},\"PeriodicalIF\":5.4000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2666667724000941/pdfft?md5=b4e82c85b1837ad5e8bce9d75dcc8758&pid=1-s2.0-S2666667724000941-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American journal of preventive cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666667724000941\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American journal of preventive cardiology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666667724000941","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/25 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
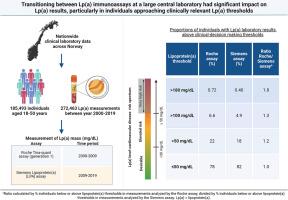
Real-world impact of transitioning from one lipoprotein(a) assay to another in a clinical setting
Background and aims
Different lipoprotein(a) [Lp(a)] assays may affect risk stratification of individuals and thus clinical decision-making. We aimed to investigate how transitioning between Lp(a) assays at a large central laboratory affected the proportion of individuals with Lp(a) result above clinical thresholds.
Methods
We studied nationwide clinical laboratory data including 185,493 unique individuals (47.7 % women) aged 18-50 years with 272,463 Lp(a) measurements using Roche (2000-2009) and Siemens Lp(a) assay (2009-2019).
Results
While the majority of individuals (66-75 %) had low levels of Lp(a) (<30 mg/dL) independent of the assay used, the Roche assay detected 20 % more individuals with Lp(a) >50 mg/dL, 40 % more individuals with Lp(a) >100 mg/dL and 80 % more individuals with Lp(a) > 180 mg/dL than the currently used Siemens assay, likely due to calibration differences.
Conclusion
Transitioning from one Lp(a) immunoassay to another had significant impact on Lp(a) results, particularly in individuals approaching clinically relevant Lp(a) thresholds.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
