Shingo Matsumoto, Alasdair D. Henderson, Li Shen, Toru Kondo, Mingming Yang, Ross T. Campbell, Inder S. Anand, Rudolf A. de Boer, Akshay S. Desai, Carolyn S.P. Lam, Aldo P. Maggioni, Felipe A. Martinez, Milton Packer, Margaret M. Redfield, Jean L. Rouleau, Dirk J. Van Veldhuisen, Muthiah Vaduganathan, Faiez Zannad, Michael R. Zile, Pardeep S. Jhund, Scott D. Solomon, John J.V. McMurray
{"title":"心力衰竭、射血分数轻度减低和保留患者使用β-受体阻滞剂的情况和预后","authors":"Shingo Matsumoto, Alasdair D. Henderson, Li Shen, Toru Kondo, Mingming Yang, Ross T. Campbell, Inder S. Anand, Rudolf A. de Boer, Akshay S. Desai, Carolyn S.P. Lam, Aldo P. Maggioni, Felipe A. Martinez, Milton Packer, Margaret M. Redfield, Jean L. Rouleau, Dirk J. Van Veldhuisen, Muthiah Vaduganathan, Faiez Zannad, Michael R. Zile, Pardeep S. Jhund, Scott D. Solomon, John J.V. McMurray","doi":"10.1002/ejhf.3383","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aims</h3>\n \n <p>In the absence of randomized trial evidence, we performed a large observational analysis of the association between beta-blocker (BB) use and clinical outcomes in patients with heart failure (HF) and mildly reduced (HFmrEF) and preserved ejection fraction (HFpEF).</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>We pooled individual patient data from four large HFmrEF/HFpEF trials (I-Preserve, TOPCAT, PARAGON-HF, and DELIVER). The primary outcome was the composite of cardiovascular death or HF hospitalization. Among the 16 951 patients included, the mean left ventricular ejection fraction (LVEF) was 56.8%, and 13 400 (79.1%) had HFpEF (LVEF ≥50%). Overall, 12 812 patients (75.6%) received a BB. The median bisoprolol-equivalent dose of BB was 5.0 (Q1–Q3: 2.5–5.0) mg with BB continuation rates of 93.1% at 2 years (in survivors). The unadjusted hazard ratio (HR) for the primary outcome did not differ between BB users and non-users (HR 0.98, 95% confidence interval [CI] 0.91–1.05), but the adjusted HR was lower in BB users than non-users (0.81, 95% CI 0.74–0.88), and this association was maintained across LVEF (<i>p</i><sub>interaction</sub> = 0.88). In subgroup analyses, the adjusted risk of the primary outcome was similar in BB users and non-users with or without a history of myocardial infarction, hypertension, or a baseline heart rate <70 bpm. By contrast, a better outcome with BB use was seen in patients with atrial fibrillation compared to those without atrial fibrillation (<i>p</i><sub>intreraction</sub> = 0.02).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>In this observational analysis of non-randomized BB treatment, there was no suggestion that BB use was associated with worse HF outcomes in HFmrEF/HFpEF, even after extensive adjustment for other prognostic variables.</p>\n </section>\n </div>","PeriodicalId":164,"journal":{"name":"European Journal of Heart Failure","volume":"27 1","pages":"124-139"},"PeriodicalIF":10.3000,"publicationDate":"2024-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Beta-blocker use and outcomes in patients with heart failure and mildly reduced and preserved ejection fraction\",\"authors\":\"Shingo Matsumoto, Alasdair D. Henderson, Li Shen, Toru Kondo, Mingming Yang, Ross T. Campbell, Inder S. Anand, Rudolf A. de Boer, Akshay S. Desai, Carolyn S.P. Lam, Aldo P. Maggioni, Felipe A. Martinez, Milton Packer, Margaret M. Redfield, Jean L. Rouleau, Dirk J. Van Veldhuisen, Muthiah Vaduganathan, Faiez Zannad, Michael R. Zile, Pardeep S. Jhund, Scott D. Solomon, John J.V. McMurray\",\"doi\":\"10.1002/ejhf.3383\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>In the absence of randomized trial evidence, we performed a large observational analysis of the association between beta-blocker (BB) use and clinical outcomes in patients with heart failure (HF) and mildly reduced (HFmrEF) and preserved ejection fraction (HFpEF).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>We pooled individual patient data from four large HFmrEF/HFpEF trials (I-Preserve, TOPCAT, PARAGON-HF, and DELIVER). The primary outcome was the composite of cardiovascular death or HF hospitalization. Among the 16 951 patients included, the mean left ventricular ejection fraction (LVEF) was 56.8%, and 13 400 (79.1%) had HFpEF (LVEF ≥50%). Overall, 12 812 patients (75.6%) received a BB. The median bisoprolol-equivalent dose of BB was 5.0 (Q1–Q3: 2.5–5.0) mg with BB continuation rates of 93.1% at 2 years (in survivors). The unadjusted hazard ratio (HR) for the primary outcome did not differ between BB users and non-users (HR 0.98, 95% confidence interval [CI] 0.91–1.05), but the adjusted HR was lower in BB users than non-users (0.81, 95% CI 0.74–0.88), and this association was maintained across LVEF (<i>p</i><sub>interaction</sub> = 0.88). In subgroup analyses, the adjusted risk of the primary outcome was similar in BB users and non-users with or without a history of myocardial infarction, hypertension, or a baseline heart rate <70 bpm. By contrast, a better outcome with BB use was seen in patients with atrial fibrillation compared to those without atrial fibrillation (<i>p</i><sub>intreraction</sub> = 0.02).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>In this observational analysis of non-randomized BB treatment, there was no suggestion that BB use was associated with worse HF outcomes in HFmrEF/HFpEF, even after extensive adjustment for other prognostic variables.</p>\\n </section>\\n </div>\",\"PeriodicalId\":164,\"journal\":{\"name\":\"European Journal of Heart Failure\",\"volume\":\"27 1\",\"pages\":\"124-139\"},\"PeriodicalIF\":10.3000,\"publicationDate\":\"2024-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3383\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3383","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Beta-blocker use and outcomes in patients with heart failure and mildly reduced and preserved ejection fraction
Aims
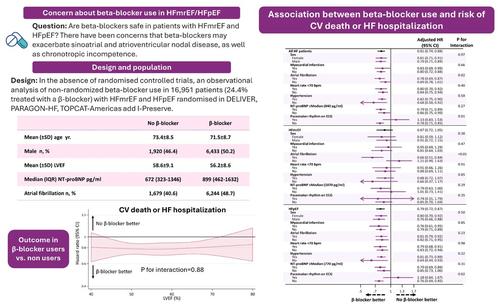
In the absence of randomized trial evidence, we performed a large observational analysis of the association between beta-blocker (BB) use and clinical outcomes in patients with heart failure (HF) and mildly reduced (HFmrEF) and preserved ejection fraction (HFpEF).
Methods and results
We pooled individual patient data from four large HFmrEF/HFpEF trials (I-Preserve, TOPCAT, PARAGON-HF, and DELIVER). The primary outcome was the composite of cardiovascular death or HF hospitalization. Among the 16 951 patients included, the mean left ventricular ejection fraction (LVEF) was 56.8%, and 13 400 (79.1%) had HFpEF (LVEF ≥50%). Overall, 12 812 patients (75.6%) received a BB. The median bisoprolol-equivalent dose of BB was 5.0 (Q1–Q3: 2.5–5.0) mg with BB continuation rates of 93.1% at 2 years (in survivors). The unadjusted hazard ratio (HR) for the primary outcome did not differ between BB users and non-users (HR 0.98, 95% confidence interval [CI] 0.91–1.05), but the adjusted HR was lower in BB users than non-users (0.81, 95% CI 0.74–0.88), and this association was maintained across LVEF (pinteraction = 0.88). In subgroup analyses, the adjusted risk of the primary outcome was similar in BB users and non-users with or without a history of myocardial infarction, hypertension, or a baseline heart rate <70 bpm. By contrast, a better outcome with BB use was seen in patients with atrial fibrillation compared to those without atrial fibrillation (pintreraction = 0.02).
Conclusions
In this observational analysis of non-randomized BB treatment, there was no suggestion that BB use was associated with worse HF outcomes in HFmrEF/HFpEF, even after extensive adjustment for other prognostic variables.
期刊介绍:
European Journal of Heart Failure is an international journal dedicated to advancing knowledge in the field of heart failure management. The journal publishes reviews and editorials aimed at improving understanding, prevention, investigation, and treatment of heart failure. It covers various disciplines such as molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, clinical sciences, social sciences, and population sciences. The journal welcomes submissions of manuscripts on basic, clinical, and population sciences, as well as original contributions on nursing, care of the elderly, primary care, health economics, and other related specialist fields. It is published monthly and has a readership that includes cardiologists, emergency room physicians, intensivists, internists, general physicians, cardiac nurses, diabetologists, epidemiologists, basic scientists focusing on cardiovascular research, and those working in rehabilitation. The journal is abstracted and indexed in various databases such as Academic Search, Embase, MEDLINE/PubMed, and Science Citation Index.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
