Iyn-Hyang Lee, Eunjung Choo, Sejung Kim, Nam Kyung Je, Ae Jeong Jo, Eun Jin Jang
{"title":"慢性阻塞性肺病患者接受初级保健的连续性与住院治疗之间的关系:基于韩国人口的队列研究。","authors":"Iyn-Hyang Lee, Eunjung Choo, Sejung Kim, Nam Kyung Je, Ae Jeong Jo, Eun Jin Jang","doi":"10.1136/bmjresp-2024-002472","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The existing evidence for the impacts of continuity of care (COC) in patients with chronic obstructive pulmonary disease (COPD) is low to moderate. This study aimed to investigate the associations between relational COC within primary care and COPD-related hospitalisations using a robust methodology.</p><p><strong>Design: </strong>Population-based cohort study.</p><p><strong>Setting: </strong>National Health Insurance Service database, South Korea.</p><p><strong>Participants: </strong>92 977 adults (≥40 years) with COPD newly diagnosed between 2015 and 2016 were included. The propensity score (PS) matching approach was used. PSs were calculated from a multivariable logistic regression that included eight baseline characteristics.</p><p><strong>Exposure: </strong>COC within primary care.</p><p><strong>Main outcome measures: </strong>The primary outcome was the incidence of COPD-related hospitalisations. Cox proportional hazard models were used to estimate HRs and 95% CIs.</p><p><strong>Results: </strong>Out of 92 977 patients, 66 677 of whom were cared for continuously by primary doctors (the continuity group), while 26 300 were not (the non-continuity group). During a 4-year follow-up period, 2094 patients (2.25%) were hospitalised; 874 (1.31%) from the continuity group and 1220 (4.64%) from the non-continuity group. After adjusting for confounding covariates, patients in the non-continuity group exhibited a significantly higher risk of hospital admission (adjusted HR (aHR) 2.43 (95% CI 2.22 to 2.66)). This risk was marginally reduced to 2.21 (95% CI 1.99 to 2.46) after PS matching. The risk of emergency department (ED) visits, systemic corticosteroid use and costs were higher for patients in the non-continuity group (aHR 2.32 (95% CI 2.04 to 2.63), adjusted OR 1.25 (95% CI 1.19 to 1.31) and exp<sup>β</sup>=1.89 (95% CI 1.82 to 1.97), respectively). These findings remained consistent across the PS-matched cohort, as well as in the sensitivity and subgroup analyses.</p><p><strong>Conclusions: </strong>In patients with COPD aged over 40, increased continuity of primary care was found to be associated with less hospitalisation, fewer ED visits and lower healthcare expenditure.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"11 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2024-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11367395/pdf/","citationCount":"0","resultStr":"{\"title\":\"Relationship between continuity of primary care and hospitalisation for patients with COPD: population-based cohort study from South Korea.\",\"authors\":\"Iyn-Hyang Lee, Eunjung Choo, Sejung Kim, Nam Kyung Je, Ae Jeong Jo, Eun Jin Jang\",\"doi\":\"10.1136/bmjresp-2024-002472\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The existing evidence for the impacts of continuity of care (COC) in patients with chronic obstructive pulmonary disease (COPD) is low to moderate. This study aimed to investigate the associations between relational COC within primary care and COPD-related hospitalisations using a robust methodology.</p><p><strong>Design: </strong>Population-based cohort study.</p><p><strong>Setting: </strong>National Health Insurance Service database, South Korea.</p><p><strong>Participants: </strong>92 977 adults (≥40 years) with COPD newly diagnosed between 2015 and 2016 were included. The propensity score (PS) matching approach was used. PSs were calculated from a multivariable logistic regression that included eight baseline characteristics.</p><p><strong>Exposure: </strong>COC within primary care.</p><p><strong>Main outcome measures: </strong>The primary outcome was the incidence of COPD-related hospitalisations. Cox proportional hazard models were used to estimate HRs and 95% CIs.</p><p><strong>Results: </strong>Out of 92 977 patients, 66 677 of whom were cared for continuously by primary doctors (the continuity group), while 26 300 were not (the non-continuity group). During a 4-year follow-up period, 2094 patients (2.25%) were hospitalised; 874 (1.31%) from the continuity group and 1220 (4.64%) from the non-continuity group. After adjusting for confounding covariates, patients in the non-continuity group exhibited a significantly higher risk of hospital admission (adjusted HR (aHR) 2.43 (95% CI 2.22 to 2.66)). This risk was marginally reduced to 2.21 (95% CI 1.99 to 2.46) after PS matching. The risk of emergency department (ED) visits, systemic corticosteroid use and costs were higher for patients in the non-continuity group (aHR 2.32 (95% CI 2.04 to 2.63), adjusted OR 1.25 (95% CI 1.19 to 1.31) and exp<sup>β</sup>=1.89 (95% CI 1.82 to 1.97), respectively). These findings remained consistent across the PS-matched cohort, as well as in the sensitivity and subgroup analyses.</p><p><strong>Conclusions: </strong>In patients with COPD aged over 40, increased continuity of primary care was found to be associated with less hospitalisation, fewer ED visits and lower healthcare expenditure.</p>\",\"PeriodicalId\":9048,\"journal\":{\"name\":\"BMJ Open Respiratory Research\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-08-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11367395/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Respiratory Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjresp-2024-002472\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002472","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
目标:现有证据表明,持续性护理(COC)对慢性阻塞性肺病(COPD)患者的影响不大。本研究旨在采用一种可靠的方法,调查初级保健中的连续性护理与慢性阻塞性肺病相关住院之间的关系:设计:基于人群的队列研究:参与者:纳入2015年至2016年期间新确诊的92 977名慢性阻塞性肺病成人(≥40岁)。采用倾向得分(PS)匹配法。PS由包含8个基线特征的多变量逻辑回归计算得出:主要结果测量:主要结果:主要结果是慢性阻塞性肺病相关住院的发生率。采用 Cox 比例危险模型估算 HRs 和 95% CIs:在 92 977 名患者中,有 66 677 人得到了基层医生的持续护理(持续护理组),26 300 人没有得到持续护理(非持续护理组)。在为期 4 年的随访期间,共有 2094 名患者(2.25%)住院治疗;其中 874 人(1.31%)来自连续性组,1220 人(4.64%)来自非连续性组。在对混杂的协变量进行调整后,非连续性组患者的入院风险明显更高(调整后 HR (aHR) 2.43 (95% CI 2.22 至 2.66))。经 PS 匹配后,这一风险略微降至 2.21(95% CI 1.99 至 2.46)。非连续性组患者的急诊就诊风险、全身使用皮质类固醇的风险和费用更高(aHR 2.32 (95% CI 2.04 to 2.63)、调整后 OR 1.25 (95% CI 1.19 to 1.31) 和 expβ=1.89 (95% CI 1.82 to 1.97))。这些结果在PS匹配队列以及敏感性和亚组分析中保持一致:结论:在 40 岁以上的慢性阻塞性肺病患者中,基层医疗服务连续性的提高与较少的住院治疗、较少的急诊就诊和较低的医疗支出有关。
Relationship between continuity of primary care and hospitalisation for patients with COPD: population-based cohort study from South Korea.
Objectives: The existing evidence for the impacts of continuity of care (COC) in patients with chronic obstructive pulmonary disease (COPD) is low to moderate. This study aimed to investigate the associations between relational COC within primary care and COPD-related hospitalisations using a robust methodology.
Design: Population-based cohort study.
Setting: National Health Insurance Service database, South Korea.
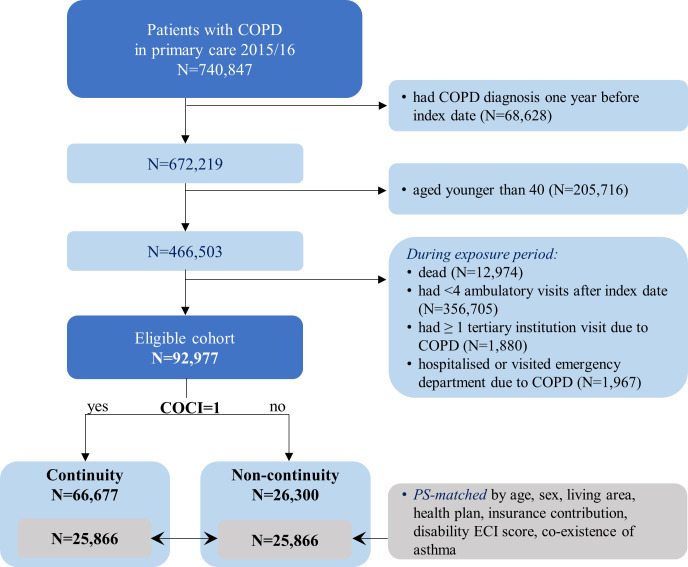
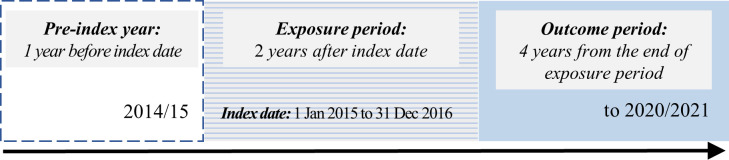
Participants: 92 977 adults (≥40 years) with COPD newly diagnosed between 2015 and 2016 were included. The propensity score (PS) matching approach was used. PSs were calculated from a multivariable logistic regression that included eight baseline characteristics.
Exposure: COC within primary care.
Main outcome measures: The primary outcome was the incidence of COPD-related hospitalisations. Cox proportional hazard models were used to estimate HRs and 95% CIs.
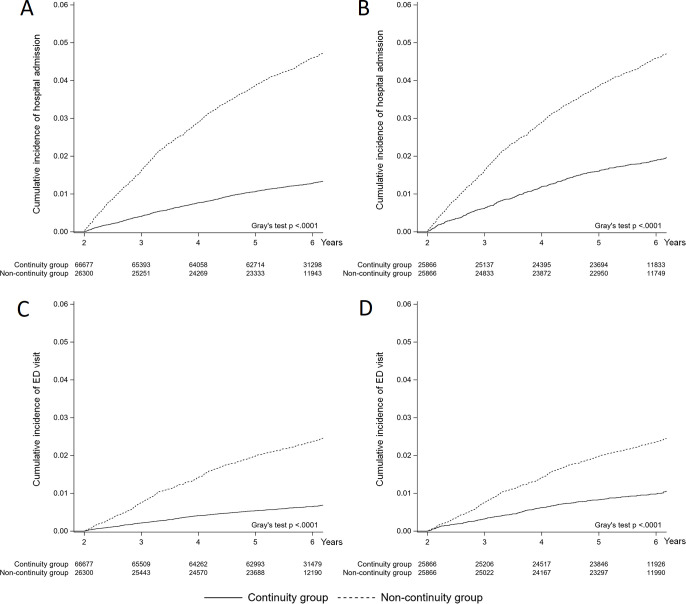
Results: Out of 92 977 patients, 66 677 of whom were cared for continuously by primary doctors (the continuity group), while 26 300 were not (the non-continuity group). During a 4-year follow-up period, 2094 patients (2.25%) were hospitalised; 874 (1.31%) from the continuity group and 1220 (4.64%) from the non-continuity group. After adjusting for confounding covariates, patients in the non-continuity group exhibited a significantly higher risk of hospital admission (adjusted HR (aHR) 2.43 (95% CI 2.22 to 2.66)). This risk was marginally reduced to 2.21 (95% CI 1.99 to 2.46) after PS matching. The risk of emergency department (ED) visits, systemic corticosteroid use and costs were higher for patients in the non-continuity group (aHR 2.32 (95% CI 2.04 to 2.63), adjusted OR 1.25 (95% CI 1.19 to 1.31) and expβ=1.89 (95% CI 1.82 to 1.97), respectively). These findings remained consistent across the PS-matched cohort, as well as in the sensitivity and subgroup analyses.
Conclusions: In patients with COPD aged over 40, increased continuity of primary care was found to be associated with less hospitalisation, fewer ED visits and lower healthcare expenditure.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
